Global Insight in Cancer Incidence, Mortality, and Disparities
DOI:
https://doi.org/10.65364/iomj.2026.02Abstract
Recent releases of cancer statistics from global agencies and national registries have provided a rather detailed and, at times, surprisingly dynamic view of how the cancer burden is shifting worldwide. The overall picture remains dominated by a steady rise in incidence, now surpassing 19 million new cases globally in 2022, while mortality approaches 10 million. At the same time, long-term improvements in high-income countries continue, especially in the United States, where more than four million deaths have been prevented since 1991. Yet these encouraging trends sit uneasily alongside emerging concerns, including rising incidence in younger adults, widening racial and regional disparities, and the long tail of diagnostic disruptions during the COVID-19 pandemic. Drawing on statistical reports from GLOBOCAN, CA: A Cancer Journal for Clinicians, population-based registries in Japan and Taiwan, and related epidemiological analyses, this review summarizes the major cancer trends observed from 2022 through 2025 and reflects on their implications for prevention, screening, and public health policy.
INTRODUCTION
Monitoring cancer patterns has always been central to understanding both the successes and failures of cancer control, and the most recent statistical cycles, from 2022 through 2025, reveal a landscape that is evolving more quickly than many expected. According to the latest GLOBOCAN estimates, the global cancer burden reached approximately 19.3 million new diagnoses and nearly 10 million deaths in 2022[1]. These patterns are consistent with estimates from the Global Burden of Disease (GBD) study, which offers complementary perspectives on cancer burden through standardized mortality, demographic decomposition, and regional comparisons across health system contexts[2]. These numbers alone hint at the accelerating pressures created by population aging and the persistence of modifiable risks.
Perhaps the more revealing details emerge from regional data, which show large and persistent gaps in survival between high- and low-income countries. A sweeping global survival analysis covering nearly 200 million patients, based on data through 2014, demonstrated that survival differences between high- and low-HDI countries remain pronounced for breast, colorectal, cervical, and childhood cancers[3]. Given the availability, completeness, and timeliness of population-based cancer registries, this review places greater emphasis on regions with mature and regularly updated surveillance systems, particularly the United States, while selectively incorporating data from Japan and Taiwan to provide comparative context. Where appropriate, global estimates are used to frame broader trends.
National data provide another layer of specificity. In the United States, the 2024 and 2025 cancer statistics reports indicate that overall mortality continues its long-term decline, while the 2025 report further quantifies age- and sex-specific shifts in incidence and highlights persistent post-pandemic disparities in screening and outcomes. Still, incidence is creeping upward for several common cancers, especially among women and younger adults[4,5]. Some of these increases, such as the rising rates of colorectal cancer in individuals under 55, have already influenced screening guidelines. Others, like the surprising shift in lung cancer incidence among women under 65, raise new questions about changing environmental and biological exposures.
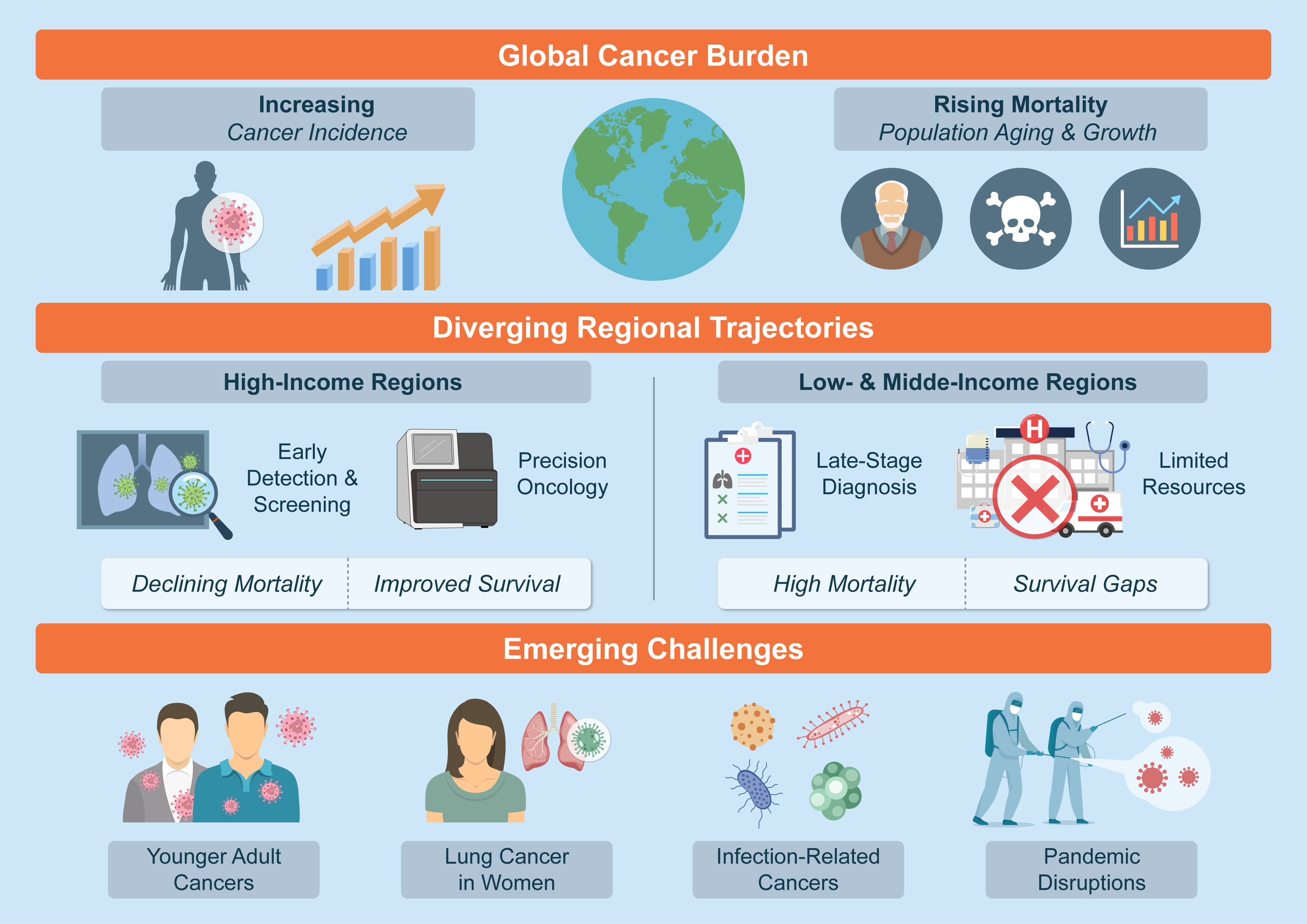
Recent global estimates published in The Lancet further reinforce this trajectory, showing that demographic ageing and population expansion are now the dominant drivers of future cancer burden, with projections indicating substantial rises across almost all world regions by 2050[6,7]. As these statistical documents accumulate, they form a comparably coherent picture: meaningful progress coexists with new epidemiological threats, and neither can be fully interpreted without an appreciation of demographic structure, regional health-system capacity, and long-standing inequities. In the sections that follow, we summarize the major tumor-specific and population-level trends reported between 2022 and 2025 and then consider how these patterns may shape future approaches to prevention, screening, and precision oncology [Figure 1].
Figure 1.Global cancer burden, regional disparities, and emerging challenges (2022–2025). Schematic overview of recent global cancer trends, highlighting the continued rise in cancer incidence and mortality driven by population aging and growth, diverging trajectories between high-income and low- and middle-income regions in terms of early detection, precision oncology, and survival outcomes, and emerging challenges including increasing cancer incidence in younger adults, rising lung cancer burden among women, infection-related cancers, and disruptions associated with the COVID-19 pandemic.
GLOBAL AND REGIONAL PATTERNS IN CANCER BURDEN
The global data from GLOBOCAN underscore how concentrated the burden remains in a handful of tumor types. Female breast cancer accounted for roughly 2.26 million cases in 2022, with lung cancer close behind at 2.21 million, followed by prostate, colorectal, and stomach cancers[1]. These tumors dominate mortality as well, particularly lung cancer, which was responsible for 1.79 million deaths. There is, however, a great deal of regional texture beneath these aggregate numbers. Eastern Asia, for instance, reported more than six million new cases, reflecting population size as well as the high prevalence of liver, stomach, and nasopharyngeal cancers in the region.
One of the more sobering observations emerging from recent analyses is the stability of the survival gap between countries at opposite ends of the socioeconomic spectrum. Despite widespread dissemination of screening and treatment advances in high-income regions, low-HDI countries show little evidence of catching up. In breast cancer alone, five-year survival remains near 90 percent in many high-income nations but often drops below 50 percent in parts of Africa[3]. Most authors attribute this to multilevel contributors, including late-stage presentation, incomplete treatment courses, and shortages of both diagnostic imaging and systemic therapies.
TRENDS IN MAJOR CANCER TYPES
Breast cancer presents a particularly illustrative example of how incidence and biology interact. The 2024 breast cancer statistics report noted a sustained increase in incidence, about 0.6 to 1 percent per year in the United States, with the rise especially noticeable among women younger than 50[8]. At the same time, recent whole-genome studies have highlighted prognostic features that are not captured by conventional pathology, such as patterns of structural variation, homologous recombination deficiency, and genome-doubling events, which may eventually refine both risk stratification and screening approaches[9].
Lung cancer trends in the most recent ACS reports are striking for a different reason. Notably, the 2025 cancer statistics report is the first to clearly document that women under 65 in the United States now have a slightly higher lung cancer incidence than men (15.7 versus 15.4 per 100,000 in 2021)[5]. The reasons remain uncertain, although several authors have pointed to a shift toward adenocarcinoma, which is less tightly linked to smoking and more commonly diagnosed in never-smokers, especially women.
Prostate cancer also appears to be entering a period of renewed epidemiological complexity. After nearly a decade of decline, U.S. prostate cancer incidence began to climb again around 2014, a trend that the 2025 cancer statistics report further attributes to continued increases in distant-stage disease[10]. Comparable findings were reported in Japan, where 94,748 new cases were diagnosed in 2019, and mortality continues to rise, particularly among men aged 85 and older[11]. The interplay between aging, PSA screening practices, and advances in imaging detection has made interpretation challenging.
Digestive cancers highlight how national policy can reshape disease trajectories. In Japan, long-term stomach and liver cancer mortality has declined, helped by population-level reductions in Helicobacter pylori infection and expanded antiviral therapy for viral hepatitis. Pancreatic cancer, by contrast, remains stubbornly lethal, its incidence rising while survival remains dismally low[12]. The United States shows a similar pattern: pancreatic cancer now causes more than 51,000 deaths annually, making it the third leading cause of cancer mortality despite being far less common than breast or lung cancer[4].
Colorectal cancer continues to draw attention because of its age-specific patterns. Incidence among individuals younger than 55 has been increasing by one to two percent each year, turning colorectal cancer into the leading cause of cancer death among young men and the second among young women in the United States[4]. The reasons are still debated, and most analyses offer a mix of dietary, environmental, and microbiome-related hypotheses.
Oral cancer statistics from Taiwan remind us how profoundly culture can influence cancer epidemiology. The combination of betel-quid chewing, smoking, and alcohol results in one of the highest male incidence rates worldwide, surpassing 30 per 100,000 in recent years[13]. Mortality has not meaningfully improved, suggesting that prevention remains the most effective intervention.
PERSISTENT DISPARITIES ACROSS POPULATIONS
The 2025 statistics for Black and African American populations in the United States provide perhaps the most compelling evidence that progress is unevenly distributed. Black individuals continue to experience the highest overall cancer mortality of any racial group in the country. Prostate, stomach, and uterine corpus cancers show mortality rates that are roughly twice those of White individuals[14]. Native American and Alaska Native populations face similarly disproportionate burdens, especially in cancers of the liver, stomach, kidney, and cervix[5]. Many of these inequalities relate to delayed diagnosis, lower screening participation, treatment access barriers, and broader structural inequities, which together contribute to persistently poorer cancer outcomes in these communities. Similar themes have been highlighted in recent Lancet analyses, which describe how widening structural and economic inequalities continue to shape both cancer incidence and mortality, particularly in lower-resource settings where diagnostic and treatment capacity remain constrained[2].
Age is emerging as another axis of disparity. Several U.S. and Japanese datasets show steep increases in cancer incidence among the elderly, particularly those over age 85, who now account for a significant and growing share of prostate, bladder, and kidney cancer diagnoses[11]. Meanwhile, young adults face their own distinct increase in incidence for colorectal, breast, and other tumors, suggesting that generational differences in lifestyle, chemical exposure, or microbiome profiles may come into play.
THE ONGOING IMPACT OF COVID-19
The pandemic left a clear imprint on cancer surveillance. Incidence fell abruptly in 2020 across nearly all major registries, a drop fully attributable to missed or delayed diagnoses rather than true reductions in cancer occurrence. The COVID-19 pandemic left a clear imprint on cancer surveillance, with sharp declines in incidence observed across major registries in 2020, reflecting delayed or missed diagnoses rather than true reductions in cancer occurrence. Updated surveillance data from the 2024 and 2025 cancer statistics reports indicate that screening volumes for several common cancers have largely rebounded toward pre-pandemic levels, although recovery has been uneven across populations, with slower normalization observed among racial and ethnic minority groups and in lower-resource settings[4]. Diagnostic backlogs persist for certain cancer types and age groups, raising concerns about stage migration and delayed treatment initiation. Consistent with these observations, earlier modeling studies predicted that colorectal cancer alone could experience between 4,000 and 7,000 excess deaths by 2040 as a downstream consequence of pandemic-related screening disruptions[5]. Recovery since 2021 has been uneven, with minority populations and low-resource regions showing slower rebounds in screening. The Annual Report to the Nation emphasized these delays and noted their potential to widen preexisting disparities if screening efforts are not strengthened[15].
FUTURE DIRECTIONS
Recent reports in The Lancet also emphasise that shifts in global risk profiles, particularly rising obesity, metabolic dysfunction, and persistent tobacco exposure in several regions, will strongly influence future cancer trajectories, reinforcing the need for coordinated prevention strategies[16-18]. Taken together, the recent statistical cycles emphasize prevention as the single most impactful strategy for reducing global cancer burden. Tobacco control and HPV vaccination remain the clearest opportunities, while alcohol moderation, hepatitis B vaccination, and elimination of betel-quid chewing could dramatically reduce incidence in particular regions. Early detection strategies are also evolving, with growing interest in risk-adapted screening for breast and prostate cancers, as well as expanded colorectal cancer screening for adults under 50.
At a population level, several of the epidemiological trends discussed above, such as rising incidence in younger adults, increasing late-stage presentation in certain cancers, and persistent survival disparities across regions, highlight the limitations of stage- and age-based risk stratification alone. In this context, advances in precision oncology offer a potential mechanistic bridge between macro-level cancer trends and individual disease biology[19,20]. Whole-genome sequencing studies suggest that structural variation patterns and mutational signatures may predict outcomes in ways that traditional staging cannot[9,21]. Whether such insights will meaningfully reduce population-level mortality, however, will depend on their accessibility, a challenge that remains substantial in low-HDI settings.
CONCLUSION
Taken together, these findings suggest several immediate priorities for cancer control. First, strengthening and harmonizing population-based cancer surveillance systems remains essential to accurately track emerging trends and disparities, particularly in under-resourced regions. Second, prevention strategies targeting modifiable risk factors, such as tobacco use, obesity, and infection-related cancers, should be intensified, with particular attention to populations experiencing rising incidence at younger ages. Third, efforts to reduce diagnostic delays and stage migration, including post-pandemic screening recovery and risk-adapted early detection, are critical to translating epidemiological gains into mortality reduction. Finally, advances in precision oncology must be coupled with policies that ensure equitable access, if genomic insights are to meaningfully impact population-level outcomes. In practice, this will require stratified implementation strategies aligned with health system capacity, ranging from comprehensive genomic profiling in high-resource settings to stepwise adoption of targeted testing, risk-based approaches, and centralized referral models in resource-constrained environments.
References
- Bray F, Laversanne M, Sung H. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin.. 2024; 74:229-63. DOI | PubMed
- GBD 2023 Demographics Collaborators. Global age-sex-specific all-cause mortality and life expectancy estimates for 204 countries and territories and 660 subnational locations, 1950-2023: a demographic analysis for the Global Burden of Disease Study 2023. Lancet.. 2025; 406:1731-810. DOI | PubMed |
- Allemani C, Matsuda T, Di Carlo V. ; CONCORD Working Group. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet.. 2018; 391:1023-75. DOI | PubMed |
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin.. 2024; 74:12-49. DOI | PubMed |
- Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin.. 2025; 75:10-45. DOI | PubMed |
- GBD 2023 Cancer Collaborators. The global, regional, and national burden of cancer, 1990-2023, with forecasts to 2050: a systematic analysis for the Global Burden of Disease Study 2023. Lancet.. 2025; 406:1565-86. DOI | PubMed |
- Bizuayehu HM, Ahmed KY, Kibret GD. Global disparities of cancer and its projected burden in 2050. JAMA Netw Open.. 2024; 7:e2443198. DOI | PubMed |
- Giaquinto AN, Sung H, Newman LA. Breast cancer statistics 2024. CA Cancer J Clin.. 2024; 74:477-95. DOI | PubMed
- Black D, Davies HR, Koh GCC. Clinical potential of whole-genome data linked to mortality statistics in patients with breast cancer in the UK: a retrospective analysis. Lancet Oncol.. 2025; 26:1417-31. DOI | PubMed
- Kratzer TB, Mazzitelli N, Star J, Dahut WL, Jemal A, Siegel RL. Prostate cancer statistics, 2025. CA Cancer J Clin.. 2025; 75:485-97. DOI | PubMed |
- Sasaki T, Higashi T, Inoue T. Urological cancer statistics on incidence from 1975 to 2019 and mortality from 1958 to 2022 in Japan. Int J Clin Oncol.. 2024; 29:1088-95. DOI | PubMed
- Higashi T, Kurokawa Y. Incidence, mortality, survival, and treatment statistics of cancers in digestive organs-Japanese cancer statistics 2024. Ann Gastroenterol Surg.. 2024; 8:958-65. DOI | PubMed |
- Yang YH. Oral cancer in Taiwan. Oral Dis.. 2025; 31:1455-66. DOI | PubMed
- Saka AH, Giaquinto AN, McCullough LE. Cancer statistics for African American and Black people, 2025. CA Cancer J Clin.. 2025; 75:111-40. DOI | PubMed |
- Sherman RL, Firth AU, Henley SJ. Annual report to the nation on the status of cancer, featuring state-level statistics after the onset of the COVID-19 pandemic. Cancer.. 2025; 131:e35833. DOI | PubMed |
- Karra P, Winn M, Pauleck S. Metabolic dysfunction and obesity-related cancer: beyond obesity and metabolic syndrome. Obesity (Silver Spring).. 2022; 30:1323-34. DOI | PubMed |
- Pati S, Irfan W, Jameel A, Ahmed S, Shahid RK. Obesity and cancer: a current overview of epidemiology, pathogenesis, outcomes, and management. Cancers (Basel).. 2023; 15:485. DOI | PubMed |
- Belladelli F, Montorsi F, Martini A. Metabolic syndrome, obesity and cancer risk. Curr Opin Urol.. 2022; 32:594-7. DOI | PubMed
- Narote S, Desai SA, Patel VP, Deshmukh R, Raut N, Dapse S. Identification of new immune target and signaling for cancer immunotherapy. Cancer Genet.. 2025; 294-295:57-75. DOI | PubMed
- Sonkin D, Thomas A, Teicher BA. Cancer treatments: past, present, and future. Cancer Genet.. 2024; 286-287:18-24. DOI | PubMed |
- Liu H, Karsidag I, Golin R, Wu G. Bridging discovery and treatment: cancer biomarker. Cancers (Basel).. 2025; 17:3720. DOI | PubMed |
Published
Issue
Section
License
Copyright (c) 2025 Hengrui Liu, Kaiyuan Hua, Joonyeon Shin, Lois Balmer, Aobing Yang, Enoch Odame Anto, Ilayda Karsidag, Florence Nakabiri, Anjellina Rukundo, Zheng Guo, walter odur (Author)

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.