Expert consensus on immune checkpoint inhibitors for non-small cell lung cancer
DOI:
https://doi.org/10.65364/iomj.2026.07Abstract
Non-small cell lung cancer (NSCLC) is the most common pathological type of lung cancer, characterized by high morbidity and mortality. Traditional treatments, including surgery, chemotherapy, and radiotherapy, have long been the mainstay of management. However, the advent of targeted therapy and immunotherapy, particularly immune checkpoint inhibitors (ICIs) such as anti-PD-1/PD-L1 antibodies, has significantly improved patient survival outcomes. These advancements have transformed the therapeutic landscape for early-stage, locally advanced, and advanced NSCLC without actionable gene mutations. Despite multiple ICIs being approved for clinical use, critical questions regarding the optimal beneficiary population and predictive biomarkers remain under investigation. To address these challenges, the Yangtze River Delta Lung Cancer Cooperation Group (ECLUNG; Youth Committee) has formulated an expert consensus on the diagnosis and treatment of NSCLC with ICIs. This consensus aims to provide standardized and evidence-based recommendations to optimize diagnostic precision and therapeutic decision-making in NSCLC.
INTRODUCTION
According to the 2024 Global Cancer Epidemiology Report, lung cancer reemerged as the most prevalent malignancy worldwide, with 2,480,675 new cases, surpassing breast cancer in incidence, and remained the leading cause of cancer-related mortality, accounting for 1,817,469 deaths[1]. In China, lung cancer consistently shows the highest incidence and mortality rates among all cancers, with 1,060,600 new cases and 733,300 deaths reported in 2022[2].
Lung cancer can be classified into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), with NSCLC being the most common subtype, accounting for 80%-85% of all cases[3]. Due to the lack of noticeable symptoms during early stages, most patients are diagnosed at an advanced stage. Meanwhile, conventional therapies (chemotherapy, surgery, radiotherapy) demonstrate suboptimal efficacy, with over 50% of surgically treated patients developing progression within 5 years and fewer than 10% of advanced-stage patients achieving five-year survival[4,5]. These therapeutic challenges highlight the need for more effective strategies to enhance both survival outcomes and quality of life in NSCLC patients.
Recently, immune checkpoint inhibitors (ICIs) have demonstrated remarkable efficacy across diverse malignancies, including NSCLC, with accumulating clinical evidence confirming significant survival benefits - particularly in advanced-stage patients who are refractory to conventional therapies. To translate these advances into clinical practice, the ECLUNG YOUNG (Yangtze River Delta Lung Cancer Cooperation Group; East China Lung Cancer Group, ECLUNG; Youth Committee) has developed an expert consensus on the diagnosis and treatment of NSCLC with ICIs. This consensus synthesizes current evidence and knowledge on the classification and mechanisms of ICIs, standardized approaches to biomarker testing and interpretation, stage-specific immunotherapy strategies, assessment of treatment response, and clinical applications of biomarkers. The ultimate goal is to optimize diagnostic precision and therapeutic decision-making, thereby improving clinical outcomes for NSCLC patients[6].
IMMUNE CHECKPOINT AND IMMUNOTHERAPY MECHANISM
The anti-tumor immune response primarily relies on the precise recognition and elimination of tumor cells by the immune system, in which T cells, natural killer (NK) cells, and macrophages function through recognizing neoantigens or abnormally expressed molecules. The activation, proliferation, and memory formation of T cells are essential for anti-tumor defense. However, tumor cells can evade immune surveillance through multiple mechanisms, including immune checkpoint pathways, antigen loss, downregulation of major histocompatibility complex (MHC) molecules, and the establishment of an immunosuppressive microenvironment. Immune checkpoint inhibitors, such as programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) and Cytotoxic T-Lymphocyte-Associated protein 4 (CTLA-4) inhibitors, represent a pivotal strategy for reversing tumor immune evasion. This therapeutic strategy effectively bridges the gap between immune surveillance and immune resistance, enabling sustained anti-tumor immunity.
The normal anti-tumor mechanisms
Under physiological conditions, the immune system operates with efficient surveillance mechanisms, that precisely identify and eliminate non-self components, including pathogens, allografts, and tumor cells. Key cells in immune responses, such as Cluster of Differentiation 8-positive (CD8+) cytotoxic T lymphocytes (CTL), NK cells, and macrophages, mediate antitumor responses through recognition of tumor-specific neoantigens or aberrantly expressed molecules, thereby initiating cytotoxic killing. During this process, T cell-mediated immunity plays a crucial role. Tumor-derived neoantigens are captured, processed, and presented by antigen-presenting cells (APCs) as peptide-MHC class I/II complexes to T cells, which then proliferate and differentiate into tumor-specific CTLs. These CTLs migrate to tumor site and specifically kill tumor cells through T cell receptor (TCR)-peptide-MHC class I interactions, while dying tumor cells release additional neoantigens to amplify the immune response. Concurrently, a subset of activated T cells differentiates into long-lived memory T cells, enabling rapid recall responses upon antigen re-exposure and ensuring sustained immune surveillance against tumors[7].
The mechanisms of tumor immune evasion
Under physiological conditions, the immune surveillance system effectively identifies and eliminates potentially malignant cells, preventing tumorigenesis. However, tumors employ multiple sophisticated mechanisms to evade immune surveillance, promoting oncogenesis and progression. Key immune evasion strategies include:
(1) Immune Checkpoint Mechanisms: Tumor cells express immunosuppressive ligands that interact with inhibitory receptors on T cells, such as PD-1, Lymphocyte Activation Gene-3 (LAG-3), T Cell Immunoglobulin and Mucin Domain Containing-3 (TIM-3), T Cell Immunoreceptor with Ig and ITIM Domains (TIGIT), V-domain Ig Suppressor of T cell Activation (VISTA), and 2B4 (CD244), thereby suppressing T cell function to facilitate immune evasion.
(2) Antigen Loss and MHC Downregulation: Tumor cells reduce or completely lose the expression of specific antigens and downregulate the expression of MHC molecules through genetic mutations or other mechanisms,impairing antigen presentation and escaping immune recognition and attack.
(3) Immunosuppressive Microenvironment: The tumor microenvironment (TME) harbors various immunosuppressive cells, such as Regulatory T cells (Tregs) and Myeloid-Derived Suppressor Cells (MDSCs), as well as immunosuppressive molecules like TGF-β and IL-10. These elements collectively create an immunosuppressive TME that suppresses effector T cell function and promotes tumor immune evasion.
Other mechanisms include abnormal costimulatory signals, dysregulated anti-apoptotic signals, and compromised host immune function. These interconnected mechanisms synergistically drive tumor immune evasion and maintain persistent oncogenic proliferation.
The mechanism of immune checkpoint inhibitors
Immune checkpoints represent critical regulatory mechanisms in the immune system that maintain self-tolerance and prevent autoimmunity through negative regulation of immune responses. Malignancies exploit these pathways to evade immune surveillance. The predominant ICIs in clinical practice are PD-1/PD-L1 inhibitors and CTLA-4 inhibitors, with their mechanistic details summarized in Table 1.
| Type | Mechanism of action | Approved drugs |
| CTLA-4 inhibitors | Expressed on activated T cells;Competitively blocks CD28/B7 costimulation to enhances early T-cell activation | IpilimumabaTremelimumab |
| PD-1 inhibitors | Negative regulatory receptor on T cells;Inhibits PD-1/PD-L1/PD-L2 signaling to restore T-cell function | NivolumabaPembrolizumabaCemiplimabToripalimababSintilimababCamrelizumababTislelizumababPenpulimababSerplulimababIvonescimababc |
| PD-L1 inhibitors | Expressed on tumor/immune cells;Prevents PD-L1/PD-1 signaling to maintain T-cell cytotoxicity | DurvalumabaAtezolizumabaSugemalimabab |
| LAG-3 inhibitors | Expressed on T/NK cells;Disrupts LAG-3-MHCII interaction to augment T-cell response | Not available |
| TIM-3 inhibitors | Expressed on T cells and other immune cells;Blocks TIM-3-ligand(Gal-9/CEACAM-1) binding to reverse T-cell exhaustion | Not available |
| TIGIT inhibitors | Coexpressed with CD226 on T/NK cells;Inhibits TIGIT-CD155 interaction to enhance NK/T-cell cytotoxicity | Not available |
PD-1/PD-L1 inhibitors
PD-1, an immunosuppressive transmembrane protein expressed on T cells, mediates immune inhibition upon binding its ligand PD-L1. Tumor cell-expressed PD-L1 engages PD-1, inducing tyrosine phosphorylation of cytoplasmic domain in T cell and subsequent recruitment of SHP-2 phosphatase. This cascade dephosphorylates TCR signaling molecules, suppressing downstream pathways and impairing T cell activation, cytokine secretion, and proliferation. PD-1/PD-L1 inhibitors block this interaction, reversing T cell suppression and restoring antitumor immunity[8].
CTLA-4 inhibitors
CTLA-4, an immune checkpoint receptor encoded by the CTLA-4 gene, is predominantly expressed on activated CD4+ and CD8+ T cells. It competes with cluster of differentiation 28 (CD28) for binding to shared ligands (CD80/CD86, collectively termed B7 molecules), exhibiting higher binding affinity. CTLA-4-B7 interaction competitively blocks CD28 co-stimulation, attenuating both TCR and CD28 signaling pathways. Additionally, CTLA-4 diminishes CD28 stimulation by either downregulating B7 expression on APCs or clearing these molecules through endocytosis. Moreover, CTLA-4 can induce dendritic cells (DCs) to express indoleamine 2,3-dioxygenase by binding to B7 on APCs, thereby inhibiting T cell function.
Other checkpoint inhibitors
LAG-3 is primarily expressed on activated T cells, NK cells, and plasmacytoid dendritic cells. Its interaction with MHC class II molecules suppresses CD4+ T cell activation. Therapeutic LAG-3 blockade potentiates T cell activity, augmenting antitumor immunity[9].
TIM-3 is another negative immune regulator and often acts in concert with PD-1 to maintain T cell tolerance. It is expressed on various immune cells, including effector T cells, regulatory T cells, and NK cells. It inhibits cell activation and proliferation by binding to specific ligands such as galectin-9 (Gal-9), carcinoembryonic antigen-related cell adhesion molecule-1 (CEACAM-1)[10,11].
TIGIT is commonly co-expressed with CD226 on T cells and NK cells. It impairs antitumor function through CD155/CD112 binding. TIGIT inhibition enhances both NK cell cytotoxicity and T cell activation, demonstrating therapeutic potential in cancer immunotherapy[12,13].
TESTING AND INTERPRETATION OF PD-L1
PD-L1 testing methodology
PD-L1 (a type I transmembrane protein) is routinely assessed via immunohistochemistry (IHC). The recommended specimens include surgically resected or biopsied tumor tissue fixed in 10% neutral buffered formalin and paraffin-embedded. When tissue is unavailable, ethanol-fixed cell blocks may serve as alternatives (with documented specimen type), though they are suboptimal for evaluating immune cell PD-L1 expression due to enumeration challenges. Decalcified bone metastases are not recommended due to artifact risks and reduced antigenicity.
For recurrent or metastatic disease, recurrent or metastatic lesion samples are preferred for PD-L1 testing. When both primary and metastatic lesion samples are available, separate PD-L1 testing and independent reporting of results are recommended to clarify the expression status at different sites. Given PD-L1’s temporal expression dynamics, testing is recommended at initial diagnosis and before changing treatment regimens. Avoid archival tissues exceeding 3 years due to potential epitope degradation[14].
PD-L1 testing must be performed using validated antibody reagents and platforms. Currently, NMPA-approved kits include 22C3, 28-8, SP142, SP263, and E1L3N, and the main testing platforms are DAKO and Ventana. Among these, SP263 and 22C3 (FDA/NMPA-approved companion diagnostics) exhibit strong concordance with 28-8, whereas SP142 demonstrates lower sensitivity, particularly in low-expressing cases.
Common reagents and platforms for PD-L1 testing in NSCLC are detailed in Table 2[15].
| Reagent | Clone | Platform | PD-1/L1 inhibitor | FDA threshold | EMA threshold | NMPA threshold | Recommendation level |
| PD-LI IHC 22C3 pharmDx | 22C3 mouse mAb | Dako Autostainer Link 48 | Pembrolizumab | CDx, TPS ≥ 1% (1L/2L) | Certified,TPS > 50% (1L)TPS > 1% (2L)** | Approved, TPS ≥ 1% (1L) | Preferred |
| Cemiplimab | TPS ≥ 50% | / | / | ||||
| 22C3 antibody reagent | Pembrolizumab | / | / | Approved, TPS > 1% (1L)(22C3 requires LDT confirmation) | |||
| PD-LI IHC28-8 pharmDx | SP288 rabbit mAb | Dako Autostainer link 48 | Nivolumab | CDx, TPS ≥ 1% (in combination with Ipilimumab) | Certified,TPS ≥ 1%,TPS ≥ 5%,TPS ≥ 10% | Approved, TPS ≥ 1% | Preferred |
| Complementary diagnostics,TPS ≥ 1%,TPS ≥ 5%,TPS ≥ 10% | |||||||
| Ventana PD-Ll(SP263) assay | SP263 rabbit mAb | Ventana BenchMark | Pembrolizumab | / | Certified,TPS > 50% (1L)TPS ≥ 1% (2L) | / | Preferred |
| Nivolumab | / | Certified,TPS ≥ 1%,TPS ≥ 5%,TPS ≥ 10% | / | ||||
| Durvalumab | / | Certified,TPS ≥ 1% | / | ||||
| Atezolizumab | CDx, TPS ≥ 1% (adjuvant therapy after surgery) | Certified,TPS ≥ 50% | Approved TPS ≥ 1% (adjuvant therapy after surgery) | ||||
| cemiplimab | CDx,TPS ≥ 50% (1L) | TPS ≥ 50% | / | ||||
| Ventana PD-Ll(SP142) assay | SP142 rabbit mAb | Ventana BenchMark | Atezolizumab | CDx, TPS ≥ 50% or IPS ≥ 10% (1L) | Certified,TPS ≥ 50% | Approved TPS ≥ 50% or IPS ≥ 10% (1L) | Recommended |
| / | 73-10 rabbit mAb | Dako Autostainer Link 48 | Avelumab | / | / | / | Not r ecommended |
| PD-LI (E1L3N) antibody | E1L3Nrabbit mAb | Leica BOND-MAX | Pembrolizumab | / | / | Approved TPS ≥ 1% (1L) | Preferred |
| Nivolumab | / | / | Approved TPS ≥ 1% (1L) | Recommended |
PD-L1 expression evaluation criteria and interpretation standards
PD-L1 expression assessment depends on the PD-L1 antibody clone, tumor histology, and intended immunotherapy agent. Current scoring systems, mainly including the tumor proportion score (TPS), immune proportion score (IPS), and combined positive score (CPS), should be applied according to manufacturer instructions and guideline recommendations. Different drugs have different testing requirements, including companion diagnostics, complementary diagnostics, or testing exemption[16]. The positive threshold for PD-L1 expression varies by antibody clone: the 22C3, 28-8, and SP263 clones define positivity as any intensity of staining in tumor cell membranous, while SP142 includes both tumor cell membranous and immune cell membranous/cytoplasmic staining. Given the semi-quantitative nature of immunohistochemical assessment, PD-L1 testing should be conducted in accredited laboratories by pathologists with specialized PD-L1 training. Using standardized protocols, pathologists evaluate specific staining patterns in tumor regions (including tumor cell membrane staining alone or combined tumor cell membrane and immune cell membrane/cytoplasmic staining) by microscopy, calculate the percentage of positive cells, and provide objective evidence to guide clinical treatment decisions.
The specific interpretation criteria for PD-L1 testing are shown in Table 3 and the current ICIs for NSCLC are listed in Table 4[14].
| PD-L1 Antibody Clone | Testing platform | Detection system | Scoring method | Positive cutoff | Clinical research threshold | PD-1/L1 inhibitor | FDA approval |
| 22C3 | DAKO Link 48 Autostainer | EnVision Flex | Percentage of TCs with membranous staining (any intensity) | TPS ≥ 1% (evaluate ≥ 100 TCs) | 1%, 50% | Pembrolizumab | Companion diagnostic |
| 28-8 | DAKO Link 48 Autostainer | EnVision Flex | Percentage of TCs with membranous staining (any intensity) | TPS ≥ 1% (evaluate ≥ 100 TCs) | 1%, 5%, 10% | Nivolumab | Complementary diagnostics |
| SP142 | Ventana BenchMark ULTRA | Optiview + amplification | TPS: Percentage of TCs with membranous staining (any intensity) IPS: Percentage of positively stained ICs in tumor area | TPS ≥ 50% or IPS ≥ 10% (evaluate ≥ 50 TCs and stroma) | TPS at 1%, 5%, and 50%;IPS at 1%, 5%, and 10%. | Atezolizumab | Companion diagnostic |
| SP263 | Ventana BenchMark ULTRA | Optiview | Percentage of TCs with membranous staining (any intensity) | TPS ≥ 1% (evaluate ≥ 100 TCs) | 1%, 25%, 50% | Durvalumab | Annotations* |
| 73-10 | DAKO Link 48 Autostainer | EnVision Flex | Percentage of TCs with membranous staining (any intensity) | TPS ≥ 1% (no minimum TC requirement) | 1% | Avelumab | Diagnostic Test |
| Drug | Target | FDA approved indications | EMA approved indications | NMPA approved indications |
| Pembrolizumab | PD-1 | 1. First-line treatment for EGFR/ALK-negative metastatic NSCLC with PD-L1 TPS ≥ 1% 2. First-line combination with carboplatin and paclitaxel (or nab-paclitaxel) for metastatic LUSC3. First-line combination with pemetrexed and platinum for metastatic non-squamous NSCLC4. Second-line monotherapy for PD-L1 TPS ≥ 1%, EGFR/ALK-negative advanced NSCLC after progression on chemotherapy5. Adjuvant monotherapy after surgery and platinum-based chemotherapy for stage IB (tumor ≥ 4 cm), II, or IIIA NSCLC6. Neoadjuvant combination with platinum-based chemotherapy, followed by adjuvant monotherapy for resectable NSCLC (tumor ≥ 4 cm or lymph node involvement) | 1. First-line treatment for EGFR/ALK-negative metastatic NSCLC with PD-L1 TPS > 50%2. First-line combination with pemetrexed and platinum for EGFR/ALK-negative metastatic non-squamous NSCLC3. First-line combination with carboplatin and paclitaxel (or nab-paclitaxel) for metastatic LUSC 4. Second-line monotherapy for EGFR/ALK-negative advanced NSCLC with PD-L1 TPS ≥ 1% | 1. First-line treatment for EGFR/ALK-negative locally advanced or metastatic NSCLC with PD-L1 TPS ≥ 1%2. First-line combination with carboplatin and paclitaxel for metastatic LUSC3. First-line combination with pemetrexed and platinum for metastatic non-squamous NSCLC. |
| Nivolumab | PD-1 | 1. First-line combination with ipilimumab and 2 cycles of chemotherapy for advanced or recurrent NSCLC2. First-line combination with ipilimumab for EGFR/ALK-negative metastatic NSCLC with PD-L1 TPS ≥ 1%3. Treatment for metastatic NSCLC after progression on platinum-based chemotherapy and other treatments4. Neoadjuvant combination with platinum-based chemotherapy for resectable NSCLC | First-line combination with ipilimumab and 2 cycles of chemotherapy for EGFR/ALK-negative metastatic NSCLC | 1. Second-line or subsequent-line monotherapy for EGFR/ALK-negative, locally advanced or metastatic NSCLC after progression on platinum-based chemotherapy 2. Neoadjuvant combination with platinum-based chemotherapy for resectable NSCLC, (particularly tumor ≥ 4 cm or lymph node involvement) |
| Cemiplimab | PD-1 | First-line treatment for NSCLC with PD-L1 TPS ≥ 50% | No indications for NSCLC currently | No indications for NSCLC currently |
| Atezolizumab | PD-L1 | First-line treatment for EGFR/ALK-negative advanced NSCLC with high PD-L1 expression (TPS ≥ 50% or IPS ≥ 10%) 2. First-line combination with nab-paclitaxel and carboplatin for EGFR/ALK-negative metastatic non-squamous NSCLC3. First-line combination with bevacizumab, paclitaxel and carboplatin for EGFR/ALK-negative advanced non-squamous NSCLC 4. Second-line treatment for metastatic NSCLC after progression on platinum-based chemotherapy5. Adjuvant monotherapy for PD-L1 TPS ≥ 1%, stage II-IIIA NSCLC after resection and platinum-based chemotherapy | 1. First-line combination with nab-paclitaxel and carboplatin for EGFR/ALK-negative metastatic non-squamous NSCLC 2. First-line combination with bevacizumab, paclitaxel and carboplatin for metastatic non-squamous NSCLC3. Adjuvant monotherapy for PD-L1 TPS ≥ 50%, high risk of recurrence, EGFR/ALK-negative, stage II-IIIA NSCLC after resection and platinum-based chemotherapy | 1. First-line monotherapy for EGFR/ALK-negative metastatic NSCLC with PD-L1 TPS ≥ 50% or IPS ≥ 10% by NMPA-approved assays2. First-line combination with pemetrexed and platinum for EGFR/ALK-negative metastatic non-squamous NSCLC3. Adjuvant monotherapy for PD-L1 TPS ≥ 1%. Stage II-IIIA NSCLC after resection and platinum-based chemotherapy |
| Durvalumab | PD-L1 | 1. Consolidation treatment for unresectable stage III NSCLC without progression after CCRT2. Combination with tremelimumab and platinum chemotherapy for EGFR/ALK-negative NSCLC | Consolidation treatment for PD-L1 TPS ≥ 1%, unresectable, locally advanced NSCLC without progression after platinum-based chemoradiotherapy | Consolidation treatment for unresectable stage III NSCLC without progression after CCRT |
| Toripalimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | 1. First-line combination with pemetrexed and platinum for EGFR/ALK-negative, unresectable locally advanced or metastatic non-squamous NSCLC2. Perioperative combination therapy followed by adjuvant monotherapy for resectable stage IIIA-IIIB NSCLC |
| Sintilimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | 1. First-line combination with pemetrexed and carboplatin for EGFR/ALK-negative advanced non-squamous NSCLCL 2. First-line combination with gemcitabine and platinum for locally advanced or metastatic squamous NSCLC without targetable genomic mutation |
| Camrelizumaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | 1. First-line combination with pemetrexed and carboplatin for EGFR/ALK-negative advanced non-squamous NSCLC2. First-line combination with paclitaxel and carboplatin for EGFR/ALK-negative advanced squamous NSCLC |
| Tislelizumaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | 1.First-line combination with pemetrexed and platinum for EGFR/ALK-negative locally advanced or metastatic non-squamous NSCLC2. First-line combination with carboplatin and paclitaxel (or nab-paclitaxel) for advanced squamous NSCLC 3. Second-line monotherapy for squamous and non-squamous NSCLC |
| Penpulimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | First-line combination with paclitaxel and carboplatin for locally advanced or metastatic squamous NSCLC |
| Serplulimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | 1. First-line combination with nab-paclitaxel and carboplatin for unresectable locally advanced or metastatic squamous NSCLC2. Treatment for unresectable or metastatic MSI-H advanced solid tumors |
| Cadonilimaba | PD-1/CTLA-4 Dual-Specific Antibodies | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Zimberelimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Pucotenlimaba | PD-1 | No indications for NSCLC currently | No indications for NSCLC currently | Treatment for unresectable or metastatic MSI-H/dMMR advanced solid tumors |
| Sugemalimaba | PD-L1 | No indications for NSCLC currently | No indications for NSCLC currently | First-line combination with pemetrexed and carboplatin for EGFR/ALK-negative metastatic non-squamous NSCLC2. First-line combination with paclitaxel and carboplatin for metastatic squamous NSCLC |
| Adebrelimaba | PD-L1 | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Envafolimaba | PD-L1 | No indications for NSCLC currently | No indications for NSCLC currently | Treatment for unresectable or metastatic MSI-H/dMMR advanced solid tumors |
| Socazolimaba | PD-L1 | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Benmelstobarta | PD-L1 | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Ivonescimaba | PD-1/VEGF Bispecific Antibodies | No indications for NSCLC currently | No indications for NSCLC currently | Combination with pemetrexed and carboplatin for EGFR-mutated locally advanced or metastatic non-squamous NSCLC after EGFR TKI failure |
| Cadonilimaba | PD-1/CTLA-4 Bispecific Antibodies | No indications for NSCLC currently | No indications for NSCLC currently | No indications for NSCLC currently |
| Ipilimumab | CTLA-4 | First-line combination with nivolumab for EGFR/ALK-negative metastatic NSCLC with PD-L1 TPS ≥ 1% | No indications for NSCLC currently | No indications for NSCLC currently |
| Tremelimumab | CTLA-4 | Combination with durvalumab and platinum for EGFR/ALK-negative metastatic NSCLC | No indications for NSCLC currently | No indications for NSCLC currently |
IMMUOTHERAPY FOR NSCLC
Resectable NSCLC
Immunotherapy for early-stage NSCLC has undergone transformative evolution, progressing from adjuvant to adjuvant therapy to neoadjuvant and perioperative therapy, from monotherapy to combinations with chemotherapy, radiotherapy, anti-angiogenic therapy, and other modalities. These advancements have significantly enriched the treatment options for resectable NSCLC, improved major pathologic response (MPR) and complete pathological response (pCR), and disease-free survival (DFS) rates. However, the optimal treatment paradigm is still under investigation. Multiple ongoing clinical trials are evaluating various perioperative immunotherapy combinations to maximize survival outcomes, Current evidence and treatment recommendations are summarized as follows.
Neoadjuvant immunotherapy
Neoadjuvant immunotherapy administered preoperatively when patients retain intact lymphatic systems, abundant tumor neoantigens, and optimal performance status, demonstrates enhanced antitumor immune activation with potential to eradicate micrometastases and reduce recurrence. Current approaches encompass immune monotherapy, dual checkpoint inhibition, chemoimmunotherapy, immuno-antiangiogenic combinations, and immuno-radiotherapy. Among these, the chemoimmunotherapy currently has the most substantial evidence.
For resectable EGFR/ALK-negative NSCLC (tumor ≥ 4 cm or node-positive) without ICI contraindications, neoadjuvant nivolumab plus platinum-based doublet chemotherapy is strongly recommended. For patients ineligible for ICIs, neoadjuvant platinum-based doublet chemotherapy is recommended.
Immune monotherapyThe phase II CheckMate-159 trial evaluated neoadjuvant nivolumab monotherapy in 21 resectable stage I-IIIA NSCLC patients, demonstrating a 45% MPR rate (9/20) in 20 surgically treated patients, with 18-month recurrence-free survival (RFS) and overall survival (OS) rates of 73% and 95% respectively[18]. Updated 5-year follow-up data in 2023 showed 5-year RFS and OS rates of 60% and 80%, with better outcomes in MPR patients (HR = 0.61) and PD-L1-positive patients (TPS ≥ 1%, HR = 0.36), where 89% (8/9) of MPR patients achieved 5-year DFS without cancer-related deaths, while the non-MPR group (n = 11) had 6 recurrences and 3 deaths[19]. Subsequent studies, including LCMC-3, IONESCO, PRINCEPS, and ChiCTR-OIC-17013726 have reported MPR rates of 6%-45% and pCR rates of 0%-15% with neoadjuvant immune monotherapy, showing relatively lower efficacy compared to combination approaches[20-23]. Therefore, for patients without treatment contraindications, combination immunotherapy is recommended as the preferred neoadjuvant approach, with monotherapy remaining an alternative option.
Dual immunotherapyThe Phase II Neostar study evaluated neoadjuvant nivolumab vs. nivolumab plus ipilimumab in 44 patients with resectable stage I-IIIA NSCLC (single-station N2). The MPR rate were 22% (5/23) with monotherapy and 38% (8/21) with combination therapy. Among surgical subgroup, the MPR rates were 24% (5/21) and 50% (8/16) respectively. The study confirmed comparable surgical feasibility and safety of both regimens, while the combination therapy provided superior efficacy, with enhanced tumor immune infiltration and memory formation[24].
Similarly, the Phase II NeoCOAST trial (n = 84, stage IA3-IIIA) revealed superior efficacy for durvalumab combinations vs. monotherapy: pCR rates increased from 3.7% (monotherapy) to 9.5-12.5% (combination with oleclumab/monalizumab/danvatirsen), while MPR rates improved from 11.1% to 19.0-31.3%, with comparable safety profiles[25].Other ongoing studies such as the Phase II Neopredict-Lung trial (nivolumab plus relatlimab, a LAG-3 inhibitor) continue exploring the feasibility of neoadjuvant dual-immunotherapy. Given the current limitation to Phase II evidence, dual-immunotherapy regimens remain investigational in the perioperative setting[26].
Immunotherapy combined with chemotherapyThe landmark Phase III CheckMate-816 trial established nivolumab plus platinum-doublet chemotherapy as the first FDA/NMPA-approved neoadjuvant regimen for resectable stage IB-IIIA/IIIB (T3N2) NSCLC (AJCC 7th, tumors ≥ 4 cm or node-positive), demonstrating superior pCR (24.0% vs. 2.2%; OR = 13.94, P < 0.001) and prolonged median event-free survival (EFS) (31.6 vs. 20.8 months; HR = 0.63, P = 0.005) vs. chemotherapy alone, with comparable grade 3-4 Treatment-Related Adverse Events(TRAEs) (33.5% vs. 36.9%)[27]. Chinese subgroup analysis revealed even greater benefit (pCR: 25.0% vs. 1.9%, OR = 11.05; mEFS: not reach vs. 13.9 months, HR = 0.47) with favorable safety.
Similarly, the Phase II TD-FOREKNOW trial demonstrated that camrelizumab-chemotherapy significantly improved pCR rates (32.6% vs. 8.9%; OR = 4.95) and MPR rates (65.1% vs. 15.6%; OR = 10.13) vs. placebo-chemotherapy in resectable stage IIIA-IIIB (only T3N2 for Stage IIIB, AJCC 8th) NSCLC, with higher R0 resection rates (92.5% vs. 85.7%) and trending survival benefit (mEFS HR = 0.52)[28].
Based on CheckMate-816 trial, neoadjuvant nivolumab-chemotherapy is strongly recommended for EGFR/ALK-negative resectable NSCLC (tumor ≥ 4 cm or node-positive) without immunotherapy contraindications.
Immunotherapy combined with anti-angiogenic therapyThe phase II EAST ENERGY trial investigated neoadjuvant pembrolizumab-ramucirumab in 24 PD-L1-positive (≥ 1% by 22C3 assay) stage IB-IIIA NSCLC patients. This two-cycle regimen achieved a 50% MPR rate (90% CI 31.9%-68.1%), meeting the primary endpoint, with 50% of MPR patients (6/12) attaining pCR. Grade 3 AEs occurred in 37.5% of patients, with no ramucirumab-related wound healing complications observed[29].
Another phase II trial of camrelizumab-apatinib in stage IIA-IIIB (T3N2-eligible) NSCLC (n = 78) demonstrated 83% R0 resection, 57% MPR, and 23% pCR rates, with only 5% grade 3-4 TRAEs[30].
While these immunotherapy-antiangiogenic combinations show promise, larger randomized trials are needed to confirm efficacy through larger-scale clinical trials.
Immunotherapy combined with radiotherapyThe single-arm phase II NCT04271384 trial (n = 25) demonstrated 80% MPR and 83% pCR rates with neoadjuvant nivolumab plus stereotactic ablative radiotherapy (SABR) in early-stage NSCLC, with 96% resection rates and favorable safety (4% grade 3-5 TRAEs)[31].
Another phase II NCT02904954 study compared stereotactic body radiotherapy (SBRT) followed by durvalumab vs. durvalumab monotherapy in patients with potentially resectable stage I-IIIA NSCLC (n = 60). The results showed that the combination group had significantly higher MPR (53.3% vs. 6.7%, P < 0.0001) and pCR (30.7% vs. 0%) rates, with comparable resection rates (both 87%) and safety profiles(grade 3-4 AEs:20% vs. 17%)[32]. Updated data in 2023 showed 3-year DFS of 65% (intent-to-treat population) and 3-year PFS of 76% (surgical cohort, n = 52), with a trend toward better PFS in the combination group (83% vs. 69%, P = 0.19)[33].
The SACTION 01 study explored the efficacy and safety of SBRT followed by tislelizumab plus chemotherapy in EGFR wild-type, resectable stage II-III NSCLC (n = 46). Results showed strong efficacy (MPR: 76.1%, pCR: 52.2%, R0 resection: 95.7%) and manageable toxicity (grade ≥ 3 AEs: 26.1%)[34]. Based on these promising results, the Phase III SACTION 2401 study is expected to commence.
While these phase II trials demonstrate promising efficacy signals in resectable NSCLC, their small sample sizes necessitate validation through larger randomized controlled studies to establish optimal treatment strategies and patient selection criteria.
Given the evidence for chemo-immunotherapy is the most compelling in the neoadjuvant setting, we recommend three cycles of PD-1/PD-L1 inhibitor plus platinum-doublet chemotherapy as the standard neoadjuvant approach for resectable NSCLC (tumors ≥ 4 cm or node-positive) without ICI contraindications, while other immune-based combinations remain investigational.
Adjuvant immunotherapy
Adjuvant immunotherapy is administered postoperatively. It helps reverse the immune suppression caused by surgery and stress, enhances antitumor immune memory, eradicates micrometastases, and reduces the risk of recurrence and metastasis.
The IMpower010 study is the first Phase III clinical trial demonstrating adjuvant immunotherapy benefit in early-stage NSCLC. The trial randomized 1,280 patients with completely resected stage IB (≥ 4 cm)-IIIA NSCLC (AJCC 7th) to receive 1-4 cycles of adjuvant chemotherapy followed by either 16 cycles of atezolizumab or best supportive care (BSC). In PD-L1 ≥ 1% subgroup, atezolizumab significantly improved DFS (median NR [Not Reached] vs. 35.3 months; HR = 0.66) with 3-year DFS rates of 60.0% vs. 48.2%. OS also showed a favorable trend (HR = 0.71), with 5-year OS rate of 76.8%[35,36]. Based on these findings, the FDA and NMPA approved atezolizumab for adjuvant immunotherapy in PD-L1 ≥ 1%, stage II-IIIA NSCLC in 2021 and 2022 respectively.
The Phase III KEYNOTE-091 study evaluated adjuvant pembrolizumab in patients with completely resected stage IB (≥ 4 cm) - IIIA NSCLC (AJCC 7th edition). Pembrolizumab met its primary endpoint, significantly improving DFS in the overall population (53.6 vs. 40.2 months; HR = 0.76) with enhanced effect in chemotherapy-treated subgroups (HR = 0.73), while maintaining an acceptable safety profile. Based on these findings, the FDA approved this regimen in 2023 for adjuvant therapy following platinum-doublet chemotherapy[37].
The aforementioned studies support adjuvant immunotherapy. For resectable NSCLC, it is recommended that patients receive 1-year ICI maintenance therapy following adjuvant chemotherapy.
Neoadjuvant and adjuvant immunotherapy (perioperative immunotherapy)
Building upon neoadjuvant/adjuvant immunotherapy success, emerging perioperative ‘sandwich’ regimens demonstrate efficacy in resectable NSCLC. For stage IIIA-IIIB, we recommend neoadjuvant toripalimab-chemotherapy followed by adjuvant toripalimab. For tumors ≥ 4 cm or node-positive disease, neoadjuvant pembrolizumab-chemotherapy with adjuvant pembrolizumab is preferred. For stage II-IIIA, neoadjuvant tislelizumab-chemotherapy plus adjuvant tislelizumab is recommended, all recommended for ICI-eligible patients after exclusion of immunotherapy contraindications.
Immune monotherapyThe Phase II LCMC3 trial (n = 181) evaluated perioperative atezolizumab with optional postoperative chemo/radiotherapy in resectable stage IB-IIIB NSCLC, demonstrating 3-year DFS and OS rates of 72% and 82% respectively in the MPR-evaluable population, Stratified analysis by disease stage revealed that the 3-year DFS rates for stage I-II and stage III were 75% and 70% respectively, while the OS rates were 82% and 81%. Adjuvant atezolizumab demonstrated superior outcomes compared to observation (3-year DFS: 83% vs. 64%, HR = 0.44; 3-year OS: 89% vs. 77%, HR = 0.48), with similar patterns in non-MPR patients (DFS HR = 0.48; OS HR = 0.50)[20].
Immunotherapy combined with chemotherapyThe KEYNOTE-671 study, which achieved dual positive endpoints in EFS and OS, evaluated perioperative pembrolizumab vs. placebo plus chemotherapy (3 neoadjuvant + 13 adjuvant cycles) in resectable stage II-IIIB NSCLC (n = 797). At a median follow-up of 36.6 months, result showed pembrolizumab significantly improved median EFS by 28.9 months (47.2 vs. 18.3 months; HR = 0.59, 95% CI 0.48-0.72), while OS showed similar improvement regardless of PD-L1 status (median OS NR vs. 52.4 months; HR = 0.72, 95% CI 0.56-0.93). Secondary endpoints also demonstrated substantial improvement in pathological responses (MPR: 32.0% vs. 11.0%, 95% CI: 13.9-24.7, P < 0.0001; pCR: 18.1% vs. 4.0%, 95% CI: 10.1-18.7, P < 0.0001). Based on these, the FDA approved pembrolizumab plus platinum-based chemotherapy as neoadjuvant therapy followed by adjuvant pembrolizumab monotherapy for resectable NSCLC (tumor ≥ 4 cm or lymph node-positive) in October 2023. This approval marked the first perioperative immunotherapy indication in early-stage NSCLC[38].
The Phase III NEOTORCH study evaluated perioperative toripalimab vs. placebo in resectable stage II-III NSCLC (EGFR/ALK wild-type for nonsquamous), using a novel “3 + 1 + 13” regimen (3 neoadjuvant chemoimmunotherapy cycles, 1 adjuvant combination, 13 maintenance monotherapy cycles). As of November 30, 2022, toripalimab met the primary endpoint (median EFS: not evaluable vs. 15.1 months; HR = 0.40, 95%CI 0.28-0.57; P < 0.001) and achieved better pathological responses, with 6-fold higher MPR (48.5% vs. 8.4%) and 25-fold higher pCR (24.8% vs. 1.0%). The R0 resection rate reached 95.8% with manageable safety[39]. These results led to NMPA approval of toripalimab in 2023 as the first China-approved and second globally-approved perioperative immunotherapy for stage IIIA-IIIB NSCLC.
The RATIONALE-315 study evaluated neoadjuvant tislelizumab or placebo plus chemotherapy (3-4 cycles) followed by adjuvant tislelizumab or placebo monotherapy (8 cycles) in EGFR/ALK wild-type, resectable stage II-IIIA NSCLC(n = 453). Results showed that tislelizumab achieved significantly higher MPR (56.2% vs. 15.0%) and pCR (40.7% vs. 5.7%) rates (both P < 0.0001), with consistent benefits across subgroups regardless of stage, histology, or PD-L1 expression[40].Updated interim analyses demonstrated significant improvement in EFS with tislelizumab (HR = 0.56, P = 0.0003) and a clinically meaningful OS trend (HR = 0.62, P = 0.0193), though OS data remain immature[41]. ELCC 2024 data further revealed comparable surgical outcomes (resection rates: 84.1% vs. 76.2%; R0 rates: 95.3% vs. 93.1%), similar operative duration or hospitalization time, and favorable safety (grade ≥ 3 postoperative complications: 11.1% vs. 15.6%) between arms[42]. Following acceptance of its perioperative indication by China’s Center for Drug Evaluation (CDE) on 2024, tislelizumab represents a promising treatment option for resectable NSCLC.
The phase III CheckMate-77T trial(n = 461) in resectable stage II-IIIB NSCLC demonstrated that perioperative nivolumab (4 neoadjuvant cycles with chemotherapy + 13 adjuvant monotherapy cycles) significantly improved EFS vs. placebo (median NR vs. 18.4 months; HR = 0.58, P = 0.00025), with consistent benefit across subgroups except never-smokers. Enhanced efficacy was observed in stage III and PD-L1-positive subgroup. Pathological responses favored nivolumab (pCR: 25.3% vs. 4.7%; MPR: 35.4% vs. 12.1%), while maintaining surgical feasibility and safety[43].
The phase III AEGEAN trial (n = 802) in resectable stage IIA-IIIB[N2] NSCLC demonstrated perioperative durvalumab (4 neoadjuvant cycles with chemotherapy + 12 adjuvant monotherapy cycles) significantly improved EFS (NR vs. 25.9 months; HR = 0.68, P = 0.0039) and pathological responses (pCR: 17.2% vs. 4.3%; MPR: 33.3% vs. 12.3%; both P < 0.0001) vs. placebo, while maintaining comparable safety. Notably, surgical feasibility remained high (R0 resection: 94.7% vs. 91.3%) despite 50% of patients having stage IIIN2 disease. This confirmed durvalumab’s dual benefit of efficacy and surgical feasibility in N2 populations[44].
The data above demonstrate that the chemo-immunotherapy significantly enhances both MPR and pCR rates, bringing substantial clinical benefits in resectable NSCLC patients.
Immunotherapy combined with anti-angiogenic therapyThe phase II ALTER-L043 trial evaluated penpulimab-based neoadjuvant/adjuvant therapy in 49 patients with resectable stage IIB-IIIB(N2) NSCLC lacking targetable gene mutations. Patients were stratified into three cohorts: Group A (neoadjuvant penpulimab + chemotherapy + anlotinib, adjuvant penpulimab + anlotinib), Group B (neoadjuvant penpulimab + chemotherapy, adjuvant penpulimab alone), and Group C (neoadjuvant penpulimab + anlotinib, adjuvant penpulimab + anlotinib). As of August 3, 2023, surgical resection rates were 87.5% (A), 87.5% (B), and 76.5% (C). Pathological responses were notable, with MPR rates of 70.0% (A), 37.5% (B), and 80.0% (C), and pCR rates of 50.0% (A), 37.5% (B), and 60.0% (C). The objective response rate (ORR) to neoadjuvant therapy was 50.0% (A), 37.5% (B), and 47.06% (C). These findings support the potential of combining PD-1 inhibition with antiangiogenic therapy as a perioperative strategy for resectable locally advanced NSCLC(LA-NSCLC)[45].
Immunotherapy combined with radiotherapyOne Phase Ib dose-escalation study (n = 9) evaluated neoadjuvant durvalumab plus chemotherapy with low-dose radiotherapy (three dose cohorts: 10 Gy/5fx, 20 Gy/10fx, 30 Gy/15fx) followed by adjuvant durvalumab in EGFR/ALK wild-type, potentially resectable stage III NSCLC. All patients achieved tumor downstaging post-neoadjuvant therapy, with an overall ORR of 66.7% and R0 resection rate of 77.8% (7/9). Pathological responses varied by cohort: Cohort 1 (10 Gy) showed 33.3% MPR and pCR; Cohort 2 (20 Gy) achieved 66.7% MPR but 0% pCR; Cohort 3 (30 Gy) attained 100% MPR and 66.7% pCR. The regimen demonstrated favorable safety with no dose-limiting toxicities (DLTs), treatment-related surgical delays, or deaths. Grade 3 AEs occurred in 33.3% of patients. The study preliminarily identified 30 Gy/15 fractions as the optimal radiotherapy dose, though further validation is needed to confirm the safety and efficacy of this combination[46].
The Phase II SAKK 16/18 trial evaluated neoadjuvant durvalumab plus chemotherapy with three radiotherapy regimens (Group A: 20 × 2 Gy; Group B: 5 × 5 Gy; Group C: 3 × 8 Gy) followed by adjuvant durvalumab in resectable cT1-4N2M0 NSCLC (n = 31). Interim analysis (data cutoff: October 8, 2022) showed an 81% surgical rate (25/31), with pCR achieved in 20% (5/25; Group B:3, C:2) and MPR in 76% (19/25; Group A:4, B:8, C:7) of resected patients. TRAEs occurred in 97% of patients, with 4% attributed to durvalumab and 4% to radiotherapy. These preliminary findings support the potential of neoadjuvant immunoradiotherapy while awaiting mature data from SAKK 16/18[47].
Notably, ongoing trials, such as IMpower030 and NCT03694236, are expected to refine immunotherapy strategies for early-stage NSCLC[48,49].
In summary, for resectable stage II–III NSCLC, current evidence (NEOTORCH, KEYNOTE-671, RATIONALE-315, CheckMate-77T, AEGEAN) supports 3-4 cycles of neoadjuvant ICI plus platinum-based chemotherapy, followed by adjuvant ICI monotherapy or one cycle of chemotherapy plus ICIs for one year.
Immunotherapy recommendations for resectable NSCLC are summarized in Table 5.
| Grade I recommendation | Grade II recommendation | Grade III recommendation | |
| Resectable NSCLC | 1. Adjuvant atezolizumab after radical surgery(IMpower010) (Stage II-IIIA, PD-L1 ≥ 1%)a2. Neoadjuvant nivolumab plus platinum-based chemotherapy (CheckMate 816) (Tumor ≥ 4 cm or lymph node involvement)a3. Perioperative toripalimab plus platinum-based chemotherapy followed by adjuvant toripalimab maintenance(NEOTORCH) (Stage IIIA-IIIB)a | 1. Adjuvant pembrolizumab after radical surgery (KEYNOTE-091) (IB [T ≥ 4 cm] - IIIA)a2. Neoadjuvant pembrolizumab plus platinum-based chemotherapy followed by adjuvant pembrolizumab (KEYNOTE-671) (Stage II-IIIB [N2])a 3. Neoadjuvant tislelizumab plus platinum-based chemotherapy, followed by adjuvant tislelizumab (RATIONALE-315) (Stage II-IIIA)a | 1. Neoadjuvant nivolumab plus platinum-based chemotherapy, followed by adjuvant nivolumab (CheckMate-77T) (Stage II-IIIB)a2. Neoadjuvant durvalumab plus platinum-based chemotherapy, followed by adjuvant durvalumab (AEGEAN) (Stage IIA-IIIB [N2])a |
Unresectable NSCLC
Radiotherapy enhances antitumor immunity by inducing immunogenic cell death (ICD) and remodeling the tumor microenvironment to promote immune cell infiltration and antigen presentation. Its systemic effects, including the abscopal effect, synergize with ICIs to overcome immune evasion and improve survival outcomes. For unresectable NSCLC, the exploration of immunotherapy is primarily focused on induction, concurrent, and consolidation strategies, with strongest evidence supporting consolidation therapy.
Specifically, for unresectable stage III NSCLC patients with a performance status (PS) of 0-1 and no ICIs contraindications, we recommend durvalumab as consolidation therapy after definitive concurrent chemoradiotherapy (CRT) without disease progression or alternatively sugemalimab consolidation after radical concurrent/sequential CRT without disease progression. For patients intolerant to concurrent CRT, sequential chemotherapy followed by definitive radiotherapy is recommended. For patients with a PS of 2, radiotherapy alone or sequential chemoradiotherapy is advised.
Consolidation immunotherapy
The Phase III PACIFIC trial (n = 731) established consolidation durvalumab as standard care for unresectable stage III NSCLC without progression after concurrent CRT(CCRT), demonstrating significant survival benefits vs. placebo (median OS: 47.5 vs. 29.1 months, HR = 0.72; median PFS: 16.9 vs. 5.6 months, HR = 0.52), with 5-year OS and PFS rates of 42.9% and 33.1%, respectively. Safety profiles were comparable between arms(grade 3-4 AEs: 29.9% vs. 26.1%; grade ≥ 3 pneumonitis: 3.4% vs. 2.6%)[50]. These results supported the FDA (2018) and NMPA (2019) approvals of consolidation durvalumab for unresectable stage III NSCLC without progression post-CCRT.
For patients intolerant to CCRT, sequential chemotherapy followed by radiotherapy represents an alternative approach. The Phase III GEMSTONE-301 (n = 381) showed consolidation sugemalimab significantly improved PFS vs. placebo (10.5 vs. 6.2 months; HR = 0.65), with consistent benefits in concurrent (15.7 vs. 8.3 months; HR = 0.71) and sequential CRT subgroups (8.1 vs. 4.1 months; HR = 0.57). While OS data remain immature, sugemalimab showed favorable survival trends with a manageable safety profile (grade ≥ 3 TRAEs: 11.4% vs. 5.6%)[51]. Based on these results, the NMPA approved consolidation sugemalimab in 2022 for unresectable stage III NSCLC without progression after concurrent or sequential CRT.
The Pacific series, including PACIFIC-R and PACIFIC-6, further validated consolidation immunotherapy in unresectable LA-NSCLC. Additionally, for patients with poor PS, chemotherapy-free regimes are under investigation in trials such as DUART (NCT04249362) and TRADE-hypo (NCT04351256)[52-55]. Meanwhile, intensified consolidation strategies are under exploration to improve outcomes. The COAST study demonstrated enhanced efficacy with durvalumab combinations (10-month PFS rates: 72.7% [monalizumab combination], 64.8% [oleclumab combination] vs. 39.2% [durvalumab alone]) without new safety signals[56]. Other ongoing trials exploring combinations of PD-1/PD-L1 inhibitors with CTLA-4i, CD73i, PARPi, and anti-angiogenic agents are also underway.
Induction immunotherapy
The AFT-16 study evaluated neoadjuvant/adjuvant atezolizumab plus CCRT in unresectable stage III NSCLC(n = 64). With a median follow-up of 25.1 months, results showed a median PFS and OS of 23.7 months and NR, with 18-month PFS and OS rate of 57% and 84% respectively. The regimen exhibited a manageable safety profile, supporting the feasibility of this combination for unresectable stage III NSCLC[57].
The retrospective EP05.01-004 study further validated that two cycles of induction chemoimmunotherapy followed by definitive CRT is feasible for bulky LA-NSCLC, showing significant tumor volume reduction and disease control[58].
Notably, disease progression during induction immunotherapy may preclude definitive CRT in some patients, highlighting the need for prospective trials to optimize induction strategies and define their clinical utility.
Concurrent immunotherapy
The Phase II NICOLAS trial evaluated nivolumab plus CCRT followed by nivolumab consolidation in LA-NSCLC(n = 79). With a median follow-up of 21 months, nivolumab gained a median PFS of 12.7 months and median OS of 38.8 months[59].
The Phase II KEYNOTE-799 study investigated pembrolizumab plus CCRT followed by pembrolizumab consolidation in unresectable stage III NSCLC. At median follow-up of 18.5 months (Cohort A, squamous/nonsquamous) and 13.7 months (Cohort B, nonsquamous), ORR were 71.4% and 75.5% with median PFS of 30.6 months and NR, respectively, demonstrating consistent benefit across PD-L1 expression levels and histological subtypes. The regimen showed manageable toxicity, supporting concurrent immunotherapy-CCRT as a potential standard[60].
A phase II trial (NCT03110978) compared immunotherapy plus SABR (I-SABR) vs. SABR alone in stage I-IIB(T ≤ 7 cm, N0M0) or isolated lung parenchymal recurrent NSLCLC(T ≤ 7 cm). At a median 33 months’ follow-up, I-SABR significantly improved 4-year EFS (77% vs. 53%; HR = 0.38, P = 0.0056), particularly in tumors ≤ 2cm (HR = 0.35, P = 0.023). Treatment-related toxicity was acceptable (no grade ≥ 3 SABR-related events; two grade 2 pneumonitis cases), supporting I-SABR as a viable option for unresectable early-stage patients, especially with small tumors (T ≤ 2 cm)[61].
Ongoing studies such as DETERRED, KEYLYNK-012, AdvanTIG-301 and CheckMate-73L are actively exploring the potential of concurrent immunotherapy in LA-NSCLC[62-65]. They will provide more evidence for protocol optimization.
In summary, for unresectable stage III NSCLC patients who have not progressed after definitive CRT, PD-L1 inhibitor consolidation therapy for 1-2 years is recommended. However, induction or concurrent immunotherapy with CRT is not currently recommended as standard practice due to insufficient evidence.
Immunotherapy recommendations for unresectable LA-NSCLC are summarized in Table 6.
| Grade I recommendation | Grade II recommendation | Grade III recommendation | |
| PS = 0-1 | 1. Durvalumab consolidation for patients without progression after definitive concurrent chemoradiotherapy (PACIFIC)2. Sugemalimab consolidation for patients without progression after concurrent or sequential chemoradiotherapy (GEMSTONE-301) | Sequential chemoradiotherapy | / |
| PS = 2 | Radiotherapy alone or sequential chemoradiotherapy | 1. Chemotherapy alone2. Targeted therapy | / |
Stage IV NSCLC without targetable genomic alterations
PD-1/PD-L1 inhibitors are first-line standards for stage IV sq-/nsq-NSCLC without targetable alterations. While ICI monotherapy benefits patients with high PD-L1 expression, combination strategies are needed for PD-L1-low/negative populations.
Clinical trial evidence consistently demonstrates that first-line immune-based combinations benefit advanced NSCLC patients across all PD-L1 expression levels. Chemoimmunotherapy, in particular, have become guideline-endorsed first-line standards regardless of PD-L1 status. The IMpower150 trial established the ABCP regimen (atezolizumab + bevacizumab + carboplatin + paclitaxel) as an effective first-line option for nsq-NSCLC, demonstrating the potential of immunotherapy-antiangiogenic combinations[66]. Dual immunotherapy (PD-1/PD-L1 inhibitors plus CTLA-4 inhibitors) has also shown PFS and OS benefits in first-line treatment and represents another viable first-line option. However, due to the early crossover observed in the survival curves of the CheckMate-227 study, dual immunotherapy is not prioritized as the first-choice treatment regimen.
Moreover, PS plays a crucial role in regimen selection. For PS 0-1 patients, combination immunotherapy is preferred when clinically and economically feasible. For PS 2 patients, both ICI monotherapy and chemoimmunotherapy may be viable options, with monotherapy preferred for its better tolerability. Compared to chemotherapy alone, ICI monotherapy demonstrates superior survival outcomes while maintaining quality of life and manageable toxicity in poor PS patients.
Advanced squamous NSCLC
First-line treatmentya) Immune monotherapyCurrent guidelines recommend pembrolizumab, atezolizumab, or cemiplimab monotherapy as first-line treatment for advanced NSCLC patients with high PD-L1 expression (TPS ≥ 50%) and no targetable genomic alterations.
The IMPOWER110 study demonstrated that atezolizumab monotherapy significantly improved PFS (HR = 0.63) and OS (HR = 0.59) in EGFR/ALK wild-type stage IV non-squamous or squamous NSCLC patients with high PD-L1 expression (TPS ≥ 50% or IPS ≥ 10%)[67].
Similarly, KEYNOTE-024 showed pembrolizumab monotherapy significantly prolonged PFS (HR = 0.50) and OS (HR = 0.63) compared to chemotherapy in treatment-naive NSCLC with PD-L1 TPS ≥ 50% and no EGFR/ALK aberrations, while demonstrating fewer grade 3-5 TRAEs (31.2% vs. 53.3%)[68,69]. KEYNOTE-042 study expanded enrollment to include patients with PD-L1 ≥ 1%. The results demonstrated that pembrolizumab provided survival benefits across all PD-L1 expression levels (HR = 0.68 for ≥ 50%, HR = 0.75 for ≥ 20%, and HR = 0.79 for ≥ 1%), with the greatest benefit observed in the PD-L1≥ 50% subgroup[70]. These results established pembrolizumab as the preferred first-line option for advanced NSCLC with PD-L1 TPS ≥ 50% and PD-L1 TPS 1%-49%.
The EMPOWER-Lung 1 study further demonstrated cemiplimab’s superiority over chemotherapy in PD-L1 ≥ 50% NSCLC (squamous/nonsquamous), with significant improvements in median OS (26.1 vs. 13.3 months; HR = 0.57) and PFS (8.1 vs. 5.3 months; HR = 0.51) at 35-month follow-up (both P < 0.0001). Notably, sequential cemiplimab-chemotherapy after progression on cemiplimab monotherapy yielded meaningful survival benefit (median OS: 15.1 months; median PFS: 6.6 months), offering a viable salvage strategy[71].
b) Immunotherapy combined with chemotherapyFor treatment-naïve metastatic NSCLC without targetable alterations, PD-1/PD-L1 inhibitors(pembrolizumab, tislelizumab, cemiplimab, atezolizumab, camrelizumab, sugemalimab, penpulimab, sintilimab, or serplulimab) combined with platinum-based chemotherapy as first-line treatment is recommended regardless of histology or PD-L1 status.
The efficacy of immune-chemotherapy combinations is also strongly supported by clinical evidence. The KEYNOTE-407 study demonstrated that first-line pembrolizumab plus chemotherapy significantly prolonged median PFS (6.4 vs. 4.8 months, HR = 0.56, P < 0.001) and OS (15.9 vs. 11.3 months, HR = 0.64, P < 0.001) with 5-year OS reaching 18.4% and consistent benefits across all PD-L1 subgroups[72,73]. Similarly, the RATIONALE-307 trial in advanced sq-NSCLC showed superior outcomes with tislelizumab-chemotherapy combinations (platinum plus either paclitaxel [arm A] or nab-paclitaxel [arm B]) vs. chemotherapy alone [arm C]), with significantly prolonged PFS by IRC assessment (7.6 months in both arm A and B vs. 5.5 months in arm C, P < 0.001 for both comparisons), along with higher ORR (72.5%/74.8% vs. 49.6%) and longer DOR (8.2/8.6 vs. 4.2 months)[74].
The CameL-sq study demonstrated significant benefits with camrelizumab plus chemotherapy vs. chemotherapy in advanced sq-NSCLC, including improved median PFS (8.5 vs. 4.9 months, P < 0.0001) and OS (NR vs. 14.5 months, P < 0.0001)[75].Updated results showed durable efficacy in combination group, with median OS reaching 27.4 months (vs. 15.5 months; HR = 0.57, P < 0.0001) and 4-year follow-up confirmed sustained survival advantages (OS 33.9%; PFS 20.5%) regardless of PD-L1 expression level[76,77]. The GEMSTONE-302 study established sugemalimab-chemotherapy’s efficacy across all histological types and PD-L1 expression levels (median OS 25.4 vs. 16.9 months, HR = 0.65), with particularly pronounced benefits in squamous histology (OS 23.3 vs. 12.2 months, HR = 0.56; ORR 70.5% vs. 46.0%)[78]. The AK105-302 trial demonstrated penpulimab’s clinical value in sq-NSCLC, improving median PFS by 2.8 months (7.0 vs. 4.2 months, HR = 0.40) without increasing grade ≥ 3 TEAEs (69% vs. 68%)[79]. The ORIENT-12 study showed that sintilimab plus gemcitabine and platinum significantly extended the median PFS (5.5 vs. 4.9 months, P < 0.00001) assessed by the Independent Review Committee (IRC). Despite 48.9% of the patients in the chemotherapy group crossed over to the sintilimab group after progression, the OS showed benefit trend (HR = 0.567, P = 0.01701) and comparable grade ≥ 3 TEAE incidence (86.6% vs. 83.1%)[80]. The ASTRUM-004 trial further expanded options with serplulimab-chemotherapy’s superior PFS (8.28 vs. 5.72 months, HR = 0.55) and manageable safety profile (grade ≥ 3 TRAEs: 35.2% vs. 32.4%)[81].
The EMPOWER Lung 3 trial confirmed cemiplimab-chemotherapy’s histology-agnostic efficacy (OS 21.1 vs. 12.9 months, HR = 0.65; PFS 8.2 vs. 5.5 months, HR = 0.55)[82].Together with the EMPOWER Lung 1 study, cemiplimab has become the second PD-1 inhibitor (after pembrolizumab) to demonstrate efficacy in both monotherapy and combination therapy for squamous and non-squamous NSCLC, leading to FDA approval for first-line advanced NSCLC[83]. Updated data revealed durable 5-year outcomes with cemiplimab monotherapy and meaningful survival benefits when adding chemotherapy after progression on cemiplimab monotherapy, providing a viable sequential treatment strategy[84].
c) Dual blockade immunotherapyDual blockade immunotherapy with or without chemotherapy has also demonstrated promising therapeutic efficacy in advanced NSCLC and can be considered as a first-line or subsequent treatment option.
The CheckMate-9LA trial demonstrated superior outcomes with first-line nivolumab-ipilimumab-chemotherapy vs. chemotherapy alone in stage IV NSCLC (median OS 15.6 vs. 10.9 months, HR = 0.66; PFS 6.7 vs. 5.0 months, HR = 0.70), with benefits observed across all PD-L1 levels and histologies[85]. In 2020, the FDA approved this regimen for first-line treatment of EGFR/ALK wild-type advanced NSCLC, although it has not yet been approved by NMPA. Similarly, the trial evaluated first-line durvalumab ± tremelimumab in metastatic NSCLC without targetable alterations. Compared to chemotherapy alone, both durvalumab-tremelimumab (D + T) and durvalumab-tremelimumab-chemotherapy (D + T + CT) significantly improved PFS (6.2 vs. 4.8 months, HR = 0.72; 5.5 vs. 4.8 months, HR = 0.74) and OS (14.0 vs. 11.7 months, HR = 0.70; 13.3 vs. 11.7 months, HR = 0.86). The limited-course tremelimumab to durvalumab-chemotherapy demonstrated meaningful clinical benefit with manageable toxicity[86]. Based on these findings, NCCN guidelines have incorporated this approach as a category 1 recommendation for advanced NSCLC. Further clinical trials of dual checkpoint inhibitor strategies are warranted to optimize treatment paradigms.
d) Patients with PS ≥ 2The aforementioned data primarily apply to patients with PS 0-1. For NSCLC patients with PS 2, standard treatment is chemo-monotherapy or platinum-based chemotherapy. When considering immunotherapy, atezolizumab monotherapy is recommended. The IPSOS study, representing the first and only global phase III trial specifically designed for NSCLC patients ineligible for platinum-based doublet chemotherapy, established atezolizumab monotherapy as a valuable treatment option for PS 2 patients. Atezolizumab showed superior OS (10.3 vs. 9.2 months; HR = 0.78, P = 0.028) and better tolerability (grade 3/4 TRAEs: 16% vs. 33%) vs. chemotherapy, along with improved quality of life measures,such as cancer-related symptom scales. These benefits were consistent across all histology and PD-L1 subgroups[87]. Based on these findings, this consensus recommends atezolizumab monotherapy as a first-line immunotherapy option for PS 2 patients ineligible for platinum-based regimens.
Treatment strategies after first-line therapy failureTreatment strategies after first-line therapy failure require careful evaluation of drug exposure duration, best response, and response duration of prior immunotherapy to determine resistance patterns (primary vs. secondary resistance) and progression patterns (oligoprogressive vs. widespread progression).
For oligoprogression after immunotherapy, the multidisciplinary team (MDT) consultation is recommended. If the patient has good PS, continuation of ICIs combined with local therapies (radiotherapy/ablation) may be considered.
A retrospective study in 2022 included 1,536 advanced NSCLC patients treated with PD-1/PD-L1 inhibitors. Among them, 20% (n = 312) achieved initial response and 9% (n = 143) developed secondary resistance, of whom 56% (80/143) experienced oligoprogression. Patients receiving local therapy (n = 57, 56 continuing ICIs) showed significantly improved OS vs. no local therapy (HR = 0.48, P = 0.04), with 13 patients remaining progression-free ≥ 2 years post-progression[88]. In 2023, another retrospective study further classified the progression patterns based on the European Organization for Research and Treatment of Cancer consensus into four types: repeat oligoprogression (oligoprogression with a history of oligometastatic disease), induced oligoprogression (oligoprogression with a history of polymetastatic disease), de-novo polyprogression (polyprogression with a history of oligometastatic disease), and repeat polyprogression (polyprogression with a history of polymetastatic disease). Result showed that patients with repeat oligoprogression benefited from local ablative therapy (next-line PFS, 6.8 vs. 3.3 months; P = 0.0135; OS, NR vs. 24.5 months; P = 0.0337), while those with induced oligoprogression benefited from continued immunotherapy (next-line PFS: 6.1 vs. 4.1 months, P = 0.0264; OS: 45.4 vs. 32.3 months, P = 0.0348)[89]. Currently, the exploration of treatment patterns for oligoprogression after immunotherapy in NSCLC is mostly based on retrospective studies[88-91]. Ongoing prospective studies, including NCT04405401, NCT03693014, and NCT04492969, are expected to provide more evidence for the optimal management of oligoprogression post-ICI therapy.
For widespread progression post-immunotherapy, the current standard treatment is second-line chemotherapy, such as docetaxel or paclitaxel. Based on relevant clinical and retrospective studies, the combination of chemotherapy and anti-angiogenic therapy can be considered. The VARGADO trial demonstrated that docetaxel plus nintedanib in patients progressing after first-line chemoimmunotherapy yielded a DCR of 72.5%, ORR of 37.5%, and PFS of 4.8 months with manageable toxicity[92]. Pooled analysis from the ALTER-L016 and ALTER-L018 studies showed that superior outcomes with anlotinib-docetaxel vs. docetaxel monotherapy (ORR: 25.0% vs. 12.9%; DCR: 82.5% vs. 45.2%; median PFS: 5.4 vs. 2.3 months; P < 0.001)[93]. A retrospective study in 2024 further suggested survival benefit with anti-angiogenic therapy post-ICI progression (HR = 0.275, P = 0.013)[90].
Currently, there is insufficient evidence to support immunotherapy rechallenge for secondary immune resistance. Studies suggest that patients with good PS (PS ≤ 1), initial ICI duration ≥ 3 months, planned ICI discontinuation and chemotherapy between ICI courses may benefit from immunotherapy rechallenge[90,94-98]. However, robust evidence identifying optimal candidates is deficient. The mechanisms of acquired resistance to ICIs are primarily categorized into six types: loss of neoantigens, defects in antigen processing, abnormalities in the interferon (IFN)-γ signaling pathway, formation of an immunosuppressive TME, expression of co-inhibitory receptors, and other signaling pathway abnormalities[99]. These resistance mechanisms inform potential therapeutic strategies including chemoimmunotherapy combination, oncolytic virus injections or neoantigen vaccines to increase antigen release; adoptive T-cell/CAR-T/CAR-NK therapies to enhance antigen recognition and T-cell infiltration; TLR9 agonists or drug targeting the IFN-γ pathway to restore IFN-γ signaling; anti-angiogenic therapy to remodel the TME, and novel ICIs to overcome co-inhibitory receptor expression[99,100].
Emerging clinical data demonstrate promising approaches in NSCLC patients who progressed after chemotherapy and ICIs. BTCRC-LUN15-029 study showed pembrolizumab plus second-line chemotherapy (gemcitabine/docetaxel/pemetrexed) extended the median PFS to 5.1 months and the median OS to 26.8 months[101]. A Phase I clinical study explored the efficacy of tumor-infiltrating lymphocytes (TILs) plus nivolumab in nivolumab-resistant NSCLC. Among 13 evaluable patients, 3 had confirmed responses (median best change, 35%), 11 experienced tumor burden reduction, and 2 achieved durable CR for 1.5 years. This autologous TIL cell therapy was found to be relatively safe and clinically active, potentially representing a new treatment strategy for metastatic lung cancer[102]. The Phase Ib study demonstrated that intratumoral injection of Vidutolimod (a TLR agonist) plus pembrolizumab had the potential to overcome PD-1 inhibitor resistance in advanced melanoma. Among 44 patients, 11 achieved ORR, with a median DOR of 19.5 months and a median PFS of 2.8 months[103]. The Phase II S1800A study combining ramucirumab with pembrolizumab showed median OS of 14.5 vs. 11.6 months (HR = 0.69) in ICI-resistant NSCLC (prior ICI ≥ 84 days)[104]. The Phase II TACTI-002 study (Part B) showed that second-line eftilagimod alpha (soluble LAG-3 protein) plus pembrolizumab achieved an ORR of 8.3% and a DCR of 33% (iRECIST). The study also reported a 50% reduction in tumor growth rate, with a median PFS of 2.1 months and a median OS of 9.9 months[105].
However, since most studies are Phase I/II trials, conclusive evidence for immunotherapy rechallenge remain premature. Therefore, for patients progressing on immunotherapy, genetic testing and MDT consultations are recommended to develop the optimal treatment strategy, with strong encouragement for clinical trial participation when available.
For ICI-naive patients, treatment selection should be guided by biomarker and genetic testing result. Nivolumab, atezolizumab, tislelizumab, or pembrolizumab (for PD-L1 TPS ≥ 1%) can be considered as subsequent treatment. Additionally, enrollment in clinical trials is strongly recommended. The CheckMate-078 trial established nivolumab’s superiority over docetaxel in chemotherapy-pretreated advanced NSCLC, demonstrating significant improvements in both median OS (12.0 vs. 9.6 months; P = 0.0006) and ORR (16.6% vs. 4.2%; P < 0.0001)[106]. Similarly, the Phase III RATIONALE-303 trial showed that tislelizumab significantly prolonged OS and PFS compared to docetaxel (median OS 16.9 vs. 11.9 months, HR = 0.66, P < 0.0001, median PFS 4.2 vs. 2.6 months, HR = 0.63, P < 0.0001) in chemotherapy-pretreated NSCLC, with manageable safety profile[107]. The KEYNOTE-010 study indicated that in PD-L1 TPS ≥ 1%, advanced NSCLC patients, subsequent-line pembrolizumab provided significant OS benefits, with 5-year OS rates of 25.0% (TPS ≥ 50%) and 15.6% (TPS ≥ 1%) vs. 8.2% and 6.5% with docetaxel, respectively[108,109]. The OAK trial subgroup analysis demonstrated atezolizumab’s superior efficacy and safety in sq-NSCLC, showing significant OS benefit (13.8 vs. 9.6 months; HR = 0.73, P = 0.0003) regardless of PD-L1 status, with fewer grade 3-4 AEs (15% vs. 43%) compared to docetaxel[110].
For patients with poor PS (PS = 3-4), best supportive care is recommended.
Advanced non-squamous NSCLC
First-line treatmenta) Immune monotherapyCurrently, pembrolizumab, atezolizumab, and cemiplimab monotherapy are recommended as first-line treatment for advanced NSCLC patients with high PD-L1 expression and no targetable genomic alterations.
The IMpower110 study demonstrated atezolizumab’s superiority over chemotherapy in PD-L1-high (TC ≥ 50% or IC ≥ 10%) EGFR/ALK wild-type NSCLC, with significant PFS (HR = 0.63) and OS benefits (20.2 vs. 13.1 months; HR = 0.59, P = 0.01) at 15.9-month median follow-up, leading to FDA (2020) and NMPA (2021) approvals for this indication[67].
Similarly, The KEYNOTE-024 study showed pembrolizumab’s durable efficacy in PD-L1 TPS ≥ 50% NSCLC with 59.9-month follow-up data revealing superior median OS (26.3 vs. 13.4 months; HR = 0.62) and unprecedented 5-year survival rates (31.9% vs. 16.3%)[69,111]. This study was the first to report 5-year survival outcomes for first-line immunotherapy in advanced NSCLC. This trial was the first to report 5-year survival outcomes for first-line immunotherapy in advanced NSCLC. These findings were extended in KEYNOTE-042, where pembrolizumab demonstrated OS benefits across PD-L1 ≥ 1%[70]. Evidence from EMPOWER-Lung 1 further supports cemiplimab’s role in PD-L1-high disease[71].
b) Immunotherapy combined with chemotherapyIn the first-line treatment of advanced nsq-NSCLC, multiple landmark clinical trials including KEYNOTE-189, CAMEL, ORIENT-11, RATIONALE-304, GEMSTONE-302, IMpower132, and CHOICE-01 have consistently demonstrated that combining ICI with platinum-based chemotherapy significantly prolongs PFS compared to chemotherapy[78,112-119]. Based on these robust clinical data, chemotherapy combined with pembrolizumab, camrelizumab, sintilimab, tislelizumab, sugemalimab, atezolizumab, or toripalimab is recommended as a priority first-line treatment for advanced nsq-NSCLC without targetable genomic alterations.
The IMpower130 trial showed atezolizumab plus nab-paclitaxel/carboplatin significantly improved both median PFS (7.0 vs. 5.5 months; HR = 0.64, P < 0.0001) and OS (18.6 vs. 13.9 months; HR = 0.79, P = 0.033) compared to chemotherapy alone, with a manageable safety profile[120]. Additionally, the IMpower150 study demonstrated that in advanced patients without targetable genomic alterations, the combination of atezolizumab, bevacizumab, carboplatin, and paclitaxel (ABCP) significantly prolonged median PFS (8.3 vs. 6.8 months, HR = 0.62, P < 0.001) and OS (19.2 vs. 14.7 months, HR = 0.78, P = 0.02) compared to the combination of bevacizumab, carboplatin, and paclitaxel (BCP)[66]. Based on these findings, the FDA approved both atezolizumab-carboplatin-paclitaxel (ACP) and ABCP as first-line treatment for metastatic nsq-NSCLC. The EMPOWER Lung 3 study regarding chemo-immunotherapy combinations in sq-NSCLC (as detailed previously) provide additional supporting evidence for this treatment paradigm.
c) Dual blockade immunotherapyThe CheckMate-9LA study demonstrated nivolumab plus ipilimumab and two cycles of chemotherapy provides clinically meaningful benefit, regardless of PD-L1 expression levels or histological type[85]. In 2020, the FDA approved this combination as first-line treatment for advanced NSCLC.
In 2023, the 6-year follow-up data from CheckMate-227 further demonstrated durable survival advantages with nivolumab-ipilimumab dual immunotherapy in EGFR/ALK wild-type advanced NSCLC, regardless of PD-L1 expression levels: in PD-L1 < 1% patients, 6-year OS rates were 16% (HR = 0.65) for dual therapy, 10% (HR = 0.79) for nivolumab monotherapy, and 5% for chemotherapy; while in PD-L1 ≥ 1% patients, the corresponding rates were 22% (HR = 0.78), 15% (HR = 0.91), and 13% respectively[121].
These findings are complemented by the POSEIDON study results (detailed previously) supporting dual checkpoint inhibition strategies. For PS 2 patients intolerant to chemotherapy, the IPSOS trial data (discussed earlier) suggest atezolizumab monotherapy represents a viable option.
Treatment strategies after first-line therapy failureFor patients with PS 0-2, treatment strategies should be individualized through comprehensive clinical assessment, with strong recommendation for clinical trial participation at any line of therapy upon disease progression. For patients who received immunotherapy, the treatment strategy is consistent with the approach as outlined previously for advanced nsq-NSCLC following first-line treatment failure. For patients who progressed after first-line chemotherapy, re-biopsy for biomarker testing is recommended. Based on the CheckMate-078, RATIONALE-303, KEYNOTE-010, and OAK studies, subsequent-line treatment may include nivolumab or tislelizumab, pembrolizumab (limited to patients with PD-L1 TPS ≥ 1%), and atezolizumab. Camrelizumab also represents a viable alternative, with a phase II study demonstrating that camrelizumab plus apatinib achieved an ORR of 30.9%, median PFS of 5.7 months, and OS of 15.5 months[106,107,109,110]. This combination showed benefits across all PD-L1 subgroups and also in patients with STK11/KEAP1 mutations[122].
Advances in immunotherapy
Combination therapies with different immune checkpoint inhibitorsRecent advances in understanding the tumor immune microenvironment and immunotherapy resistance mechanisms have spurred development of novel ICIs targeting LAG-3, TIGIT, and TIM-3.
Eftilagimod alpha (E) is a soluble LAG-3 protein that binds to MHC II molecules, mediating the activation of APCs and CD8 T cells. The Phase II TACTI-002 study explored the combination of Eftilagimod alpha with pembrolizumab in two parts: Part A evaluated first-line treatment for metastatic NSCLC, while Part B assessed second-line treatment for PD-1/L1-inhibitor-resistant NSCLC. In Part A(n = 114), the ORR by iRECIST was 28.1% for PD-L1-negative patients, 45.5% for PD-L1 ≥ 1%, 41.7% for PD-L1 1%-49%, and 52.6% for PD-L1 ≥ 50%, along with median PFS of 6.9 months (all patients), 8.4 months (PD-L1 ≥ 1%), and 11.8 months (PD-L1 ≥ 50%)[123].The second-line cohort (Part B) achieved more modest outcomes (ORR 8.3%, DCR 33%, median PFS 2.1 months, OS 9.9 months)[105,124]. In 2022, the FDA granted Fast Track designation to Eftilagimod alpha plus pembrolizumab for first-line treatment of stage IIIB/IV NSCLC with PD-L1 TPS ≥ 1%. Other LAG-3 antibodies, such as relatlimab and LAG-525, are also undergoing Phase I/II clinical trials in melanoma and solid tumors.
TIGIT is an immune checkpoint molecule primarily expressed on T/NK cells. It inhibits immune responses by binding to its ligands. Phase I trial of vibostolimab (anti-TIGIT) demonstrated limited single-agent activity (ORR 3%) in PD-1/L1-resistant advanced NSCLC in the MK-7684-001 trial[125]. However, the phase II CITYSCAPE trial revealed significantly enhanced efficacy when combining tiragolumab (anti-TIGIT) with atezolizumab vs. atezolizumab monotherapy in PD-L1-positive disease, with improved ORR (31% vs. 16%) and PFS (5.42 vs. 3.58 months)[126]. Based on these findings, the FDA granted Breakthrough Therapy designation in 2021 to tiragolumab plus atezolizumab as first-line therapy for EGFR/ALK wild type metastatic NSCLC with high PD-L1 expression. Additional TIGIT inhibitors, including BMS-986207 and domvanalimab (AB-154), remain under investigation in preclinical and early-phase clinical development.
TIM-3, expressed across multiple immune cell subsets including T cells and innate immune cells (dendritic cells, NK cells, monocytes, and macrophages), serves as a regulator of T-cell exhaustion and tumor immune evasion. The phase I NCT03099109 trial evaluating LY3321367 (anti-TIM-3) with or without PD-L1 blockade in PD-1/L1-resistant patients showed modest clinical activity (ORR 4%, DCR 42%) but demonstrated mechanistic proof-of-concept through increased CD8+ T-cell infiltration in 50% of paired tumor biopsies[127]. This finding supports TIM-3’s role in overcoming PD-1 resistance, with several TIM-3 inhibitors (cobolimab, sabatolimab) currently in development as potential components of immunotherapy combinations for NSCLC.
Bispecific antibody immunotherapyRecent advances in bispecific antibody development have yielded promising results across multiple targets in NSCLC, including PD-1/VEGF, PD-1/CTLA-4, PD-L1/TGF-β, and PD-L1/CTLA-4.
Ivonescimab (AK112) is a PD-1/VEGF bispecific antibody that simultaneously targets PD-1 and VEGF-A, inhibiting tumor angiogenesis and modulating the TME to achieve antitumor effects. The AK112-201 study evaluated AK112 plus chemotherapy in treatment-naïve advanced NSCLC without targetable genomic alterations (Cohort 1), immunotherapy-progressed advanced NSCLC without targetable genomic alterations (Cohort 3), and EGFR-TKI-resistant advanced NSCLC with targetable genomic alterations (Cohort 2). Results showed that the ORR were 53.5% (23/43) in Cohort 1, 68.4% (13/19) in Cohort 2, and 40.0% (8/20) in Cohort 3. The median PFS was NR, 8.5 months and 7.5 months correspondently[128]. The HARMONi-A study further showed AK112 plus chemotherapy reduced progression risk by 54% (median PFS 7.1 vs. 4.8 months) and death risk by 20% (median OS 17.1 vs. 14.5 months) vs. chemotherapy alone in EGFR-mutant NSCLC post-TKI failure[128,129]. Notably, the phase III HARMONi-2 trial presented at 2024 WCLC showed ivonescimab monotherapy significantly outperformed pembrolizumab in PD-L1 ≥ 1% NSCLC (mPFS 11.1 vs. 5.8 months, HR = 0.51, P < 0.0001), representing the first immune agent to demonstrate superiority over pembrolizumab in a head-to-head phase III trial. Although not yet globally approved for NSCLC, Ivonescimab has shown significant potential in this area[130].
Other promising bispecifics include QL1706 (PD-1/CTLA-4), KN046 (PD-L1/CTLA-4) and SHR-1701 (PD-L1/TGF-β). A Phase II study showed QL1706 plus chemotherapy ± bevacizumab in treatment-naïve advanced NSCLC patients without targetable genomic alterations achieved an ORR of 45% and a median PFS of 6.8 months, with enhanced activity in EGFR-TKI resistant patients (ORR 54.8%, mPFS 8.5 months)[131]. Another Phase II clinical trial showed KN046 plus chemotherapy as first-line treatment for metastatic NSCLC achieved an ORR of 46.0%, a median PFS of 5.8 months, and a median OS of 26.6 months[132]. A Phase I study explored SHR-1701 in advanced NSCLC patients in three cohorts: treatment-naïve patients with PD-L1 TPS ≥ 1% (Cohort 1), EGFR-mutant patients with TKI resistance (Cohort 2), and immunotherapy-refractory patients with ≤ 3 prior lines of therapy (Cohort 3). The study showed promising antitumor activity across all cohorts, with ORR of 36.8%, 19.5%, and 9.1%, respectively. The median PFS was 5.3 months, 1.4 months, and 2.1 months, and the median OS was 24.2 months, 14.4 months, and 16.1 months, respectively. The safety profile was favorable, providing new treatment insights for treatment-naïve, EGFR-TKI resistance, and immunotherapy resistance NSCLC[133]. Ongoing investigations like the TRAILBLAZE study continue to explore bispecific antibodies in unresectable stage III NSCLC, further expanding the therapeutic landscape.
Immunotherapy combined with antiangiogenic therapy/targeted therapyBy reversing the immunosuppressive TME, antiangiogenic agents demonstrate synergistic potential when combined with ICIs, yielding enhanced clinical outcomes beyond additive effects (1 + 1 > 2). In addition to the IMpower150 and ORIENT-31 studies, multiple clinical trials continue to investigate this strategic combination[66,134].
The phase II S1800A study demonstrated this potential in ICI-resistant NSCLC, with ramucirumab plus pembrolizumab improving median OS to 14.5 vs. 11.6 months for standard of care (HR = 0.69)[104]. Similarly, updated results from COSMIC-021 showed cabozantinib-atezolizumab outperformed cabozantinib alone in ICI-pretreated nsq-NSCLC (median PFS 4.5 vs. 3.4 months; OS 13.8 vs. 9.4 months), with tumor shrinkage observed in 76% of patients and responses across all PD-L1 subgroups[135]. Additional promising combinations under investigation include JVDF (ramucirumab/pembrolizumab), NCT03083041 (apatinib/camrelizumab) and NCT03628521 (anlotinib/sintilimab)[136-138]. These findings align with earlier successes in IMpower150 (atezolizumab/bevacizumab/chemotherapy) and ORIENT-31 (sintilimab/bevacizumab/chemotherapy), supporting continued exploration of this strategy[66,134].
Despite promising results, not all combinations have succeeded. High-profile trials such as CONTACT-01 (atezolizumab/cabozantinib), LEAP-006/008 (pembrolizumab/lenvatinib ± chemotherapy), SAPPHIRE (sitravatinib/nivolumab), and KN046-302 (KN046/lenvatinib) failed to meet primary endpoints in ICI-pretreated NSCLC[139-142]. These mixed outcomes highlight the need for refined patient selection, optimized dosing, and predictive biomarkers to identify responders.
Immunotherapy combined with an ADCRecent advancements in antibody-drug conjugate (ADC) therapeutics have revolutionized treatment paradigms for NSCLC, with Trophoblast cell surface antigen 2 (TROP2) and HER2 ADC being most extensively studied.
TROP2, a transmembrane glycoprotein critically involved in tumor cell self-renewal and proliferation, demonstrates significant overexpression across multiple epithelial malignancies including NSCLC (64% of adenocarcinomas, 75% of squamous cell carcinomas), breast, cervical, and urothelial cancers[143,144]. Its elevated expression correlates with ICI resistance in advanced NSCLC, driving the clinical development of TROP2 ADC such as sacituzumab govitecan, datopotamab deruxtecan (Dato-DXd), and SKB264[145].
Promising results from the EVOKE-02 trial demonstrated first-line sacituzumab govitecan plus pembrolizumab achieved ORRs of 69% (PD-L1 ≥ 50%) and 44% (PD-L1 < 50%), with 6-month DoR rate of 88% in advanced NSCLC[146]. These findings are being further evaluated in the phase III EVOKE-03 study for PD-L1-high metastatic NSCLC (TPS ≥ 50%). Similarly, the TROPION-Lung02 showed Dato-DXd combinations achieved ORRs of 38% (doublet with pembrolizumab) and 49% (triplet with chemotherapy), with median PFS of 8.3 and 7.8 months respectively, in advanced NSCLC without targetable genomic alterations. Notably, Dato-DXd combinations also showed promising benefit in first-line treatment, with the ORR of 50% and 57% respectively[147]. Based on these findings, the TROPION-Lung07 and TROPION-Lung08 studies are ongoing to explore this regime (Dato-DXd + pembrolizumab ± chemotherapy) in advanced NSCLC with PD-L1 TPS < 50% and ≥ 50%, respectively[148,149]. The phase Ib TROPION-Lung04 study further validated this approach, showing ORRs of 47.4% (Dato-DXd + durvalumab) and 71.4% (triplet with chemotherapy) in treatment-naïve or previously treated, EGFR/ALK wild type advanced NSCLC, leading to the ongoing phase III AVANZAR trial comparing this regimen against pembrolizumab-chemotherapy in first-line treatment of advanced NSCLC[150]. Meanwhile, the phase II OPTITROP-Lung01 trial of SKB264 plus KL-A167 (anti-PD-L1) also showed impressive activity and manageable safety profile, with a phase III evaluation (NCT06170788) now underway[151].
For HER2-altered NSCLC, trastuzumab deruxtecan (T-DXd) has established a new standard of care in later-line settings based on DESTINY-Lung01/02/05 trials, with current investigations (DESTINY-Lung03, NCT04042701) exploring its potential in first-line combinations with durvalumab/chemotherapy or pembrolizumab for HER2-overexpressing or HER2-mutant disease[122,152,153]. These developments collectively underscore the potential of ADCs in NSCLC therapeutics across multiple molecular subsets and treatment lines.
The recommended immunotherapy options for stage IV NSCLC without targetable genomic alterations are presented in Table 7.
| Grade I recommendation | Grade II recommendation | Grade III recommendation | ||
| Squamous cell carcinoma | First-linePS = 0 ~ 1 | 1. Atezolizumab (limited to TPS ≥ 50% or IPS ≥ 10%) (IMPOWER110)2. Pembrolizumab (TPS ≥ 50%, PD-L1 TPS 1%-49%) (KEYNOTE-024, KEYNOTE-042)3. Paclitaxel/nab-paclitaxel + platinum + pembrolizumab (KEYNOTE-407) or tislelizumab (RATIONALE-307)4. Paclitaxel + platinum + camrelizumab (CameL-sq) or sugemalimab (GEMSTONE-302) or penpulimab (AK105-302)5. Gemcitabine + platinum + sintilimab (ORIENT-12)6. Nab-paclitaxel + platinum + serplulimab (ASTRUM-004) | 1. Cemiplimab (PD-L1 TPS ≥ 50%) (EMPOWER-Lung 1) 2. Paclitaxel + platinum + cemiplimab (EMPOWER-Lung 3) | 1. Nivolumab + ipilimumab + 2 cycles paclitaxel-platinum (CheckMate 9LA) 2. Durvalumab + tremelimumab + gemcitabine/paclitaxel/nab-paclitaxel + platinum (POSEIDON) |
| First-linePS = 2 | Atezolizumab monotherapy (IPSOS) | |||
| Second-line | MDT consultationParticipation in clinical trialsFor prior PD-1/L1 inhibitor use: Chemotherapy (± antiangiogenic therapy)No prior PD-1/L1 inhibitor use:1. Nivolumab (CheckMate-078)2. Tislelizumab (RATIONALE-303) | No prior PD-1/L1 inhibitor use:1. Pembrolizumab (limited to PD-L1 TPS > 1%) (KEYNOTE-010)2. Atezolizumab (OAK) | For oligoprogression: consider ICIs + local therapy (radiotherapy/ablation) | |
| Third-line | MDT consultation Participation in clinical trialsFor no prior PD-1/L1 inhibitor use: Nivolumab (CheckMate-078) | |||
| Non-squamous cell carcinoma | First-linePS = 0 ~ 1 | 1. Atezolizumab (TC ≥ 50% or IC ≥ 10%) (IMpower 110)2. Pembrolizumab (limited to TPS ≥ 50%, TPS 1%-49%) (KEYNOTE-024, KEYNOTE-042) 3. Pemetrexed + platinum + Pembrolizumab (KEYNOTE-189) or Camrelizumab (CAMEL) or Sintilimab (ORIENT-11) or Tislelizumab (RATIONALE-304) or Atezolizumab (IMpower132) or Sugemalimab (GEMSTONE 302) or Toripalimab (CHOICE-01) | 1. Paclitaxel + carboplatin + bevacizumab + atezolizumab (IMpower 150)2. Nab-paclitaxel + carboplatin + atezolizumab (IMpower 130)3. Cemiplimab (PD-L1 TPS ≥ 50%) (EMPOWER-Lung 1) 4. Pemetrexed/paclitaxel + platinum + cemiplimab (EMPOWER-Lung 3) | 1. Nivolumab + ipilimumab+ 2 cycles paclitaxel/platinum (CheckMate 9LA)2. Durvalumab + tremelimumab + gemcitabine/paclitaxel/nab-paclitaxel + platinum (POSEIDON) |
| First-linePS = 2 | Atezolizumab (IPSOS) | |||
| Second-line | MDT consultation Participation in clinical trialsFor prior PD-1/L1 inhibitor use: Chemotherapy (± antiangiogenic therapy).No prior PD-1/L1 inhibitor use:1. Nivolumab (CheckMate-078)2. Tislelizumab (RATIONALE-303) | No prior PD-1/L1 inhibitor use:1. Pembrolizumab (TPS > 1%) (KEYNOTE-010)2. Atezolizumab (OAK) | For oligoprogression: consider ICIs + local therapy (RT/ablation) | |
| Third-line | MDT consultation Participation in clinical trialsNo prior PD-1/L1 inhibitor use:1. Nivolumab (CheckMate-078)2. Tislelizumab (RATIONALE-303) | |||
Immunotherapy for advanced NSCLC with targetable genomic alterations
In NSCLC, targetable genomic alterations include EGFR-sensitive mutations, EGFR exon 20 insertions, ALK fusions, ROS1 fusions, MET exon 14 skipping mutations, RET fusions, NTRK fusions, KRAS mutations, BRAF mutations, HER2 mutations, NRG1 fusions, and FGFR alterations. For patients harboring these alterations, targeted therapy is the preferred first-line option when approved agents are available. Anti-angiogenic therapy can also be considered in combination with targeted therapy. Oligoprogression during targeted therapy may warrant local therapies while maintaining the current targeted regimen, whereas widespread progression necessitates MDT consultation and potential re-biopsy to elucidate resistance mechanisms.
Importantly, the treatment strategy should be tailored based on the patients’ condition, characteristics of the TME and clinical trial evidence. Additionally, sequential use of targeted therapies and ICIs requires vigilant monitoring for overlapping toxicities (e.g. hepatotoxicity, pneumonitis), with washout periods calculated based on the preceding drug’s half-life (typically five half-lives), organ function recovery, and disease progression pattens to optimize safety-efficacy balance[154].
EGFR mutations
For EGFR-mutant NSCLC, tyrosine kinase inhibitors (TKIs) remain the standard first-line therapy due to the tumors’ low immunogenicity and non-inflammatory microenvironment, which limit immunotherapy efficacy. Early studies have explored various immunotherapy strategies, including ICI monotherapy, ICI-chemotherapy, and ICI-TKI combinations. However, these strategies have shown limited benefits in treatment-naive patients. In CheckMate-012 study, nivolumab monotherapy (ORR 14%, mPFS 1.8 months, mOS 18.8 months) and nivolumab-chemotherapy (ORR 17%, mPFS 4.8 months, mOS 20.5 months) showed modest activity but higher toxicity (21% vs. 12% discontinuation rates) in EGFR-mutant NSCLC(n = 13)[155]. The TATTON trial (durvalumab-osimertinib) was halted due to safety concerns, with a 35% incidence of interstitial lung disease (ILD) vs. 2%-3% with osimertinib or durvalumab alone. In terms of efficacy, the ORR was 82% in 11 treatment-naive patients and 43% in 23 patients who had previously received EGFR-TKIs[156]. Multiple studies have shown that ICI monotherapy or ICI-chemotherapy are far less effective than standard EGFR-TKI therapy in treatment-naive NSCLC. Moreover, In ICI-TKI combinations, the significant toxicity risk, particularly pulmonary toxicity, often outweighs the marginal efficacy gains. Thus, ICI-TKI combinations are not recommended, and EGFR-TKIs remain the preferred first-line approach.
Although EGFR-TKIs demonstrate remarkable efficacy in EGFR-mutant NSCLC, acquired resistance inevitably develops, necessitating re-biopsy to identify resistance mechanisms and guide subsequent therapy. For EGFR-TKI resistant patients with oligoprogression or central nervous system progression, continuation of the EGFR-TKIs with local treatment may be considered. For widespread progression, in the absence of effective targeted therapies or traditional treatments, re-biopsy, MDT consultation and ICI-based strategies may be considered.
Emerging evidence suggests potential roles for various immunotherapy approaches in the EGFR-TKI-resistant NSCLC, including combinations of ICIs with chemotherapy, ICIs with antiangiogenic agents, or ICI monotherapy, though optimal sequencing and patient selection criteria require further investigation.
The IMpower150 study demonstrated improved outcomes with atezolizumab-bevacizumab-chemotherapy (ABCP) vs. bevacizumab-chemotherapy (BCP) in EGFR-mutant NSCLC (mOS 29.4 vs. 18.1 months; HR = 0.60), including TKI-pretreated subgroups (mOS 27.8 vs. 18.1 months; HR = 0.74)[157].
Subsequent ORIENT31 trial further supported the potential benefit of immunotherapy-antiangiogenic-chemotherapy combinations in EGFR-TKI-pretreated patients, showing sintilimab-IBI305-chemotherapy significantly prolonged mPFS vs. chemotherapy (6.9 vs. 4.3 months; HR = 0.46, P < 0.0001)[134]. A meta-analysis indicated that the immunotherapy-antiangiogenic-chemotherapy triplet regimen showed the best PFS outcomes compared to immunotherapy-chemotherapy (HR 0.71, 95% CI: 0.59-0.85), immunotherapy alone (HR 0.30, 95% CI: 0.22-0.41), and non-immunotherapy strategies including antiangiogenic-chemotherapy (HR 0.76, 95% CI: 0.58-1.00) or chemotherapy alone (HR 0.54, 95% CI: 0.45-0.64). However, triplet regimen showes increased toxicity compared to chemotherapy[158]. These findings collectively suggest potential clinical benefit of chemotherapy-antiangiogenic-immunotherapy combinations in EGFR-TKI-resistant patients.
Additionally, the MARIPOSA and MARIPOSA2 studies further expand therapeutic options with amivantamab-lazertinib (first-line) and amivantamab-chemotherapy (second-line) regimens for EGFR-sensitive mutant NSCLC[159,160].
In summary, while immunotherapy is not recommended as first-line treatment for EGFR-mutant NSCLC, it may be considered in specific clinical scenarios following comprehensive evaluation. When targeted therapies are unavailable or upon development of widespread resistance to EGFR-TKIs, management should commence with tissue re-biopsy to characterize resistance mechanisms. Subsequent treatment planning requires multidisciplinary assessment incorporating tumor molecular profiling, immune microenvironment biomarkers, patient performance status, treatment tolerance, and socioeconomic considerations. The selection of immunotherapy-based regimens (including ICI-chemotherapy-antiangiogenic combinations, ICI-platinum doublets, or ICI-antiangiogenic therapy) should be guided by molecular resistance patterns and determined through MDT discussion to optimize therapeutic outcomes while mitigating toxicity risks.
EGFR exon 20 insertion mutations
EGFR exon 20 insertion mutations (EGFR exon20ins) represent 5% to 12% of all EGFR mutations, demonstrating a distinct geographic distribution with lower prevalence in Chinese (4.8%-5.1%) vs. Western populations (9%-12%)[161]. These mutations exhibit remarkable molecular heterogeneity, with over 100 identified variants primarily clustering in the 761-775 peptide segment. This localization disrupts critical C-helix and loop structures, conferring intrinsic resistance to conventional EGFR TKIs[162].
Current treatment strategies for EGFR exon20ins mutations primarily involve platinum-based chemotherapy. ICI monotherapy has shown limited efficacy, while the combination of ICIs and chemotherapy appears promising but remains controversial. Kirchner et al. found that TME with EGFR exon20ins mutations are more likely to be “cold” microenvironment, characterized by a lack of cytotoxic T cells and Th1 cells[163]. Liu et al. also demonstrated that a more immunosuppressive TME in EGFR exon20ins mutations compared to wild-type, showing reduced infiltrating CD8+ FOXP3- T cells, tumor-promoting T cell phenotypes with enhanced epithelial-mesenchymal transition (EMT) capacity, and predominant M2-like macrophage infiltration[164]. This suggests that immune monotherapy may be insufficient, and combination immunotherapy could be a better option[164].
These biological features may explain the limited efficacy observed with ICI monotherapy (ORR 4%, mPFS 2.6 months) compared to chemotherapy (ORR 39%, mPFS 6.9 months)[165]. While platinum-based chemotherapy remains the therapeutic cornerstone, recent evidence suggests potential benefits from chemoimmunotherapy combinations, with one 2024 study reporting superior PFS (10.3 vs. 6.3 months, P = 0.013) and ORR (33.3% vs. 15%, P = 0.0168) vs. chemotherapy alone[166]. However, the clinical utility of ICIs remains controversial, as demonstrated by Choudhury et al. who found no significant improvement in time to treatment discontinuation (TTD) with ICIs compared to chemotherapy[167].
Moreover, the therapeutic landscape has evolved significantly with the development of mutation-specific agents. Frontline options now include amivantamab-chemotherapy (PAPILLON trial) and sunvozertinib (WU-KONG1/15), while later-line settings feature sunvozertinib (WU-KONG6) and amivantamab monotherapy (CHRYSALIS trial)[168-171].
In summary, according to the 2024 NCCN guidelines, treatment for advanced NSCLC with EGFR exon20ins mutations still refers to the strategies for advanced NSCLC without targetable genomic alteration[172]. Platinum-based chemotherapy combinations remain the cornerstone of first-line therapy, with sunvozertinib representing a viable alternative when accessible. For subsequent-line treatment, sunvozertinib is the preferred option when available. The incorporation of immunotherapy should be determined through MDT evaluation, incorporating comprehensive assessment of individual patient characteristics, tumor biomarker profiles, and immune microenvironment features to optimize therapeutic decision-making.
ALK fusion
Treatment-naïve ALK (Anaplastic Lymphoma Kinase)-rearranged NSCLC is characterized by low tumor mutational burden (TMB), sparse TILs in the TME, and diminished expression of immunostimulatory biomarkers, collectively predicting poor response to ICIs. The ImmunoTarget study reported complete lack of efficacy for ICI monotherapy in ALK-positive patients (ORR 0%)[173]. Similar to observations in EGFR-mutant NSCLC, combining ICIs with ALK-TKIs showed only marginal efficacy benefits while significantly increasing toxicity risks, particularly with crizotinib or ceritinib-based combination[174]. Therefore, ICIs are not recommended for the treatment of ALK-positive NSCLC. Moreover, the immunomodulatory effects of ALK-TKIs on the TME remain incompletely understood, though evidence suggests ALK fusions are associated with inherently low tumor immunogenicity and non-inflammatory microenvironments that may be further suppressed by ALK-TKI treatment[158]. Current data on immunotherapy for ALK-TKI-resistant patients, derived primarily from small retrospective studies, demonstrate consistently poor outcomes: ICI monotherapy yields ORRs of 0%-3.6% with PFS of 2-3 months, while ICI-chemotherapy combinations show modest improvement (ORR 28%, PFS 2.9 months)[172,175-177]. These findings collectively indicate limited clinical benefit. Therefore, immunotherapy is not recommended for treatment-naïve or TKI-resistant ALK-positive NSCLC[174].
ROS1 fusion
ROS1 (c-ros oncogene 1) fusion-positive NSCLC exhibits low immunogenicity. Although ROS1 shares high homology with ALK, the efficacy of PD-1/PD-L1 inhibitors in ROS1-positive patients differs from that in ALK-positive patients. Studies have shown that ROS1 fusion tumors have higher PD-L1 positivity rates compared to driver-negative NSCLC (46.7% vs. 36.6%), suggesting that ROS1-positive NSCLC may potentially benefit from immunotherapy[173]. The ImmunoTarget study reported an ORR of 17% with ICI monotherapy in seven ROS1-positive patients while a larger multicenter retrospective analysis (n = 184) observed an ORR of 13% and median TTD of 2.1 months among 28 patients receiving ICI monotherapy. Notably, the combination of ICIs with chemotherapy (n = 11) demonstrated significantly improved efficacy (ORR 83%, TTD 10 months), indicating that chemoimmunotherapy may offer greater clinical benefit in this population[173]. However, given the limited and retrospective nature of current evidence, immunotherapy is not routinely recommended for treatment-naïve or TKI-resistant ROS1-positive NSCLC. First-line therapy should prioritize ROS1-targeted agents such as crizotinib or entrectinib, while platinum-based chemotherapy (with or without bevacizumab) remains the standard approach after TKI failure[174]. Patients are also encouraged to participate in clinical trials to explore new therapeutic options.
MET aberrations
MET (Mesenchymal-Epithelial Transition factor) aberrations in NSCLC primarily occur as three distinct molecular subtypes: MET exon 14 skipping mutations, MET gene amplification, and protein overexpression. MET exon 14 skipping mutations occur in 3%-4% of lung cancer, while primary MET amplification is observed in 1%-5% of cases, and secondary MET amplification varies between 5%-50% of EGFR-TKI-resistant tumors depending on the TKI generation[173,179]. Currently, 4 MET-TKIs (glumetinib, bozitinib, tepotinib, and savolitinib) are approved in China exclusively for MET exon 14 skipping mutations, with no targeted therapies available for other MET alterations.
Clinical evidence demonstrates that MET-TKIs achieves ORR of 66.7%-68% in treatment-naïve patients and 41%-51.9% in in pretreated populations with MET exon 14 skipping mutations, while patients with high-copy MET amplification (≥ 10) may benefit from crizotinib, capmatinib, or tepotinib[172,180-182].
Preliminary research has revealed that MET exon 14 skipping mutation tumors exhibit lower TMB compared to unselected NSCLC, along with higher TME heterogeneity that may partially demonstrate inflammatory characteristics, with PD-L1 expression levels being independent of TMB[154,183,184].
Current evidence for immunotherapy in MET-altered NSCLC derives predominantly from retrospective analyses. The IMMUNOTARGET study involving 36 MET-altered patients (23 with exon 14 skipping mutations) demonstrated an ORR of 16%, median PFS of 3.4 months, and median OS of 18.4 months with subsequent-line ICI monotherapy[173]. Another study of 24 patients with MET exon 14 skipping mutation reported 17% ORR and 1.9-month median PFS with ICIs ± chemotherapy[183]. Notably, in MET-amplified NSCLC (n = 278), ICI monotherapy showed superior efficacy vs. chemotherapy (median OS 19 vs. 8 months, P < 0.0001), particularly in cases with copy number < 10[185].
Based on current evidence, MET-TKIs remains the first-line standard for MET-altered NSCLC. Upon development of TKI resistance or when targeted therapies are inaccessible, MDT consultation is recommended to guide subsequent treatment based on the resistance mechanisms. When no effective options exist, immunotherapy may be cautiously considered after comprehensive evaluation of patient’s physical condition, financial situation, and preferences, Subsequent therapies could refer to the treatment strategy of stage IV NSCLC with or without targetable genomic alteration.
RET fusion
RET (Rearranged during Transfection) genomic alterations include RET mutations and fusions, with RET fusions being more common in lung cancer, accounting for 1%-2% of lung adenocarcinomas[186]. Currently approved targeted therapies for RET fusions in China include pralsetinib and selpercatinib. Like other oncogenic fusions, RET fusions demonstrate low immunogenicity[174]. A study by Lee et al. evaluating various systemic therapies in 59 RET fusion NSCLC(using the multikinase inhibitor vandetanib as targeted therapy) showed pemetrexed-based chemotherapy achieved better outcomes (ORR 63.0%, mPFS 9.0 months [95% CI: 6.9-11.2], mOS 24.1 months [95% CI: 15.2-33.0]), while PD-1/PD-L1 inhibitors demonstrated limited efficacy (ORR 7.7%, mPFS 2.1 months [95% CI: 1.6-2.6], mOS 12.4 months [95% CI: 2.9-21.8])[187]. A phase 3 clinical trial demonstrated superior efficacy of selpercatinib compared to chemotherapy ± immunotherapy, with significantly prolonged PFS (24.8 vs. 11.2 months; HR 0.46; P < 0.001) and higher ORR (84% vs. 65%) among advanced RET fusion-positive NSCLC[188]. Given these data, the efficacy of first-line immunotherapy RET fusion-positive NSCLC requires further validation. When available, targeted therapy should be prioritized. If access to RET inhibitors is limited, platinum-based chemotherapy with pemetrexed may be considered[189]. The role of ICIs in this population remains undefined due to insufficient evidence, underscoring the need for additional clinical investigations to establish evidence-based therapeutic approaches[174].
KRAS mutations
KRAS(Kirsten Rat Sarcoma Viral Oncogene Homolog)-mutant NSCLC represents a distinct molecular subset with available targeted therapies including KRAS G12C inhibitors (sotorasib, adagrasib, garsorasib) and emerging KRAS G12D inhibitors (HRS-4642, MRTX-1133)[190,191]. Comparative analysis of 4,017 targetable genomic alteration-positive NSCLC samples revealed that KRAS-mutant tumors exhibit higher TMB (median 7.8 mut/Mb, n = 2,240), increased PD-L1 expression, and greater TIL levels vs. EGFR-mutant or ALK-fusion patients. Further analysis of 231 surgical specimens demonstrated KRAS-mutant tumors had enhanced T-cell infiltration (P = 0.003) and higher PD-L1+/TIL+ co-positivity rates (P = 0.007) compared to KRAS wild-type tumors, indicating KRAS mutations correlate with heightened tumor immunogenicity and an inflammatory microenvironment that may confer potential benefit from ICIs[192]. Multiple clinical and retrospective studies have demonstrated that KRAS-mutated patients can benefit from ICIs monotherapy or in combination with chemotherapy. Clinical evidence from trials including IMpower150, KEYNOTE-189, and KEYNOTE-042 support the efficacy of first-line ICIs in KRAS-mutated NSCLC[193-195]. The CheckMate 057 (n = 62) and OAK (n = 59) trials specifically showed ICI monotherapy improved OS vs. docetaxel in previously treated KRAS-mutant NSCLC[110,192,196].
Current treatment paradigms for KRAS-mutant NSCLC primarily incorporate immunotherapy-based approaches, either as monotherapy or combined with chemotherapy, with emerging evidence suggesting KRAS mutational status significantly influences therapeutic outcomes. A retrospective analysis by Amanam et al. involving 60 NSCLC patients (87% stage IV adenocarcinoma, 78% KRAS exon 12 mutations) demonstrated numerically improved median OS in the immunotherapy-treated subgroup (33 vs. 22 months, P = 0.31)[197]. However, the relationship between KRAS mutations and immunotherapy response is complex as highlighted by Dong et al.[198]. KRAS mutations coexpressed with other types of gene mutations may affect the efficacy of immunotherapy.
Specifically, KRAS frequently co-occurs with TP53 or STK11 mutations in lung adenocarcinoma, creating distinct biological and clinical phenotypes.
KRAS/TP53 co-mutated tumors exhibit elevated PD-L1 expression and may benefit from anti-PD-1 therapy (ORR ~ 30%). Conversely, when KRAS co-mutates with STK11, the efficacy of immunotherapy may be suboptimal[199]. A retrospective study analyzed the outcomes of immunotherapy in 174 patients with KRAS-mutated lung adenocarcinoma. The findings indicated that patients with only KRAS mutations had better responses to immunotherapy. Patients with KRAS/TP53 co-mutations had the greatest OS benefit (with an ORR of approximately 30%), while those with KRAS/STK11 co-mutations had the least benefit[200]. This suggests that KRAS/TP53 co-mutation may serve as a potential predictive biomarker for guiding immunotherapy. Additionally, STK11 plays a crucial role in cellular metabolism, growth, and the regulation of cell polarity. STK11 mutations are associated with the formation of an immunologically “cold” TME. Clinical data demonstrate KRAS/STK11 co-mutated adenocarcinoma have shorter PFS and OS following ICIs vs. STK11 wild-type[201]. Animal studies further confirmed that STK11 deficiency promotes resistance to PD-1/PD-L1 inhibitors. Ricciuti et al.[202] and Jeong et al.[203] also demonstrated that STK11 mutations are associated with poorer outcomes in immunotherapy for KRAS-mutated lung adenocarcinoma. Moreover, KRAS mutations encompass multiple subtypes, and the correlation between each subtype and immunotherapy efficacy is inconsistent. Further advancements in basic and clinical research are anticipated to elucidate these relationships.
In summary, the relationship between KRAS mutations and the PD-1 signaling pathway in NSCLC is complex. Most scholars currently believe that KRAS-mutated NSCLC have higher PD-L1 expression levels and they may derive better outcomes from immunotherapy compared to KRAS wild-type NSCLC. This suggests that KRAS mutations could be an important predictive biomarker for immunotherapy in NSCLC. Optimal treatment selection should involve comprehensive genomic profiling and multidisciplinary evaluation to integrate molecular findings with clinical factors, particularly for patients with STK11 co-mutations or other biomarkers of immunosuppression. As the understanding of KRAS biology evolves, ongoing clinical trials are expected to further refine precision immunotherapy approaches for this molecular subset.
BRAF V600 mutation
BRAF alterations (including mutations, deletions, and fusions) occur in 1%-5% of NSCLC cases and are classified into three functional categories based on their signaling mechanisms and kinase activity: Class I (V600D/E/K/R mutations with monomeric kinase activity, where V600E accounts for > 90% of V600 variants); Class II (G464E/V/R, G469A/V/S, L597Q/R/S/V mutations with dimer-independent kinase activity; and Class III (impaired kinase activity mutations that signal through C-RAF dimerization).
While targeted therapies have demonstrated efficacy for Class I BRAF mutations, no prospective studies have specifically evaluated immunotherapy in BRAF-mutant NSCLC. Notably, BRAF mutations, particularly BRAF non-V600 mutations, are associated with elevated TMB and PD-L1 expression[157]. Several retrospective studies have suggested that these patients may benefit from ICIs[204-206]. For BRAF V600E-mutant patients, clinical trials including NCT01336634 and PHAROS support first-line use of BRAF/MEK inhibitor combinations (dabrafenib plus trametinib or encorafenib plus binimetinib)[207,208]. Upon disease progression, MDT consultation is recommended to guide subsequent therapy, which may follow treatment guidelines for NSCLC without targetable genomic alterations. For BRAF non-V600 mutations, where neither targeted therapies nor immunotherapies have been prospectively evaluated, treatment decisions should be made through MDT discussion may consider referring to therapeutic strategies for advanced NSCLC without targetable genomic alterations.
HER2 mutations
HER2 (Human Epidermal Growth Factor Receptor 2) alterations primarily include HER2 mutations (1.6%-3%), gene amplifications (2%-4%), and protein overexpression (7.7%-15.4%). While no targeted therapies are currently approved for HER2-altered NSCLC, the FDA granted approval in August 2022 to trastuzumab deruxtecan (T-DXd, DS-8201) for previously treated HER2-mutant cases based on Phase II trial results demonstrating an ORR of 55%, a median PFS of 8.2 months, and a median OS of 17.8 months[153]. Notably, DS8201 has not yet been approved for NSCLC indications in China.
HER2-mutant tumors exhibit high immunogenicity with complex, heterogeneous TME[209]. While several small retrospective studies suggest that HER2-mutant NSCLC may benefit from ICIs-based treatment strategies, prospective studies with more robust evidence is needed to validate the conclusion[173]. ccording to the 2024 NCCN guidelines, for HER2-mutant NSCLC, we recommend referring to the treatment strategies for stage IV NSCLC without targetable genomic alterations, while incorporating MDT consultations to optimize therapeutic decision-making[171].
NTRK fusion
NeuroTrophin Receptor Kinase (NTRK), a member of the tyrosine receptor kinase family, comprises NTRK1, NTRK2, and NTRK3 genes, which encode TRKA, TRKB, and TRKC proteins respectively[152]. NTRK gene fusions, occurring in less than 5% of NSCLC cases, represent a rare but clinically important molecular subset due to their remarkable sensitivity to targeted therapies[210,211]. The fusion partners are highly diverse, and NTRK fusions are mutually exclusive with other major targetable genomic alterations[212]. Currently, entrectinib and larotrectinib constitute first-line standard of care for NTRK fusion-positive NSCLC based on their demonstrated efficacy, though detection challenges persist given the complexity of NTRK fusion identification[212,213].
The immunological characteristics and responsiveness to immunotherapy in this population remain poorly defined due to extreme rarity, with available evidence limited to case reports and small series. Dudnik et al. reported limited activity of ICIs in two NTRK-mutant patients (median PFS NR [range 3.2-NR] and the OS from diagnosis was only 4.8 months)[214]. Zhang et al. described one patient with an NCOR2-NTRK1 fusion who had high TMB (58.58 mut/Mb) and PD-L1 expression (20%-0%). The patient progressed on first-line camrelizumab but achieved significant tumor shrinkage and eventual disappearance of lesions after switching to larotrectinib[215]. The retrospective analysis by Rosen et al. (n = 76, across 17 tumor types) demonstrated modest efficacy of non-TRK inhibitor therapies (median PFS 9.6 months), with chemotherapy showing superior activity (ORR 63%) compared to ICIs, Notably, among 12 patients treated with ICIs, only one with MSI-H colorectal cancer responded[216]. Gatalica et al. suggested that TRK inhibitors alone or in combination with ICIs could be a viable treatment option[217]. Suh et al. found that larotrectinib may offer substantial gains in life expectancy and quality-adjusted life years (QALY) compared to ICIs[218].
Given this evidence, targeted therapy remains the first-line recommendation for patients with NTRK fusions. In cases where targeted therapies are unavailable or resistance develops, MDT consultation is recommended and treatment strategies should follow the guidelines for stage IV NSCLC without targetable genomic alterations, as outlined in the 2024 NCCN guidelines[218]. Following comprehensive MDT discussion, immunotherapy combined with chemotherapy may be considered cautiously as part of antitumor strategy.
NRG1 fusions
Neuregulin 1 (NRG1), a neuroregulatory growth factor capable of binding HER3 and HER4 to activate the ErbB signaling pathway, belongs to the EGF ligand family and represents a rare molecular target. The incidence of NRG1 fusions in NSCLC is 0.3%, with a rate of 0.26% in lung adenocarcinoma and 0.21% in squamous cell carcinoma. Notably, in mucinous adenocarcinoma (a rare subtype of lung adenocarcinoma), the incidence of NRG1 fusions is significantly higher, reaching up to 7%[213]. Current targeted therapies under investigation for advanced pan-cancer NRG1 fusions include afatinib, pyrotinib, zenocutuzumab (MCLA-128), and seribantumab, with preliminary data showing promising efficacy[219].
Zenocutuzumab (MCLA-128), a bispecific antibody targeting HER2 and HER3, has demonstrated an ORR of 34%, with tumor shrinkage observed in up to 70% of patients and a median DOR of 14.9 months (95% CI: 7.4-20.4). The 12-month DOR rate was 57% (95% CI: 34-75%)[220]. The immunological characteristics of NRG1 fusion-positive tumors appear unfavorable for immunotherapy, as evidenced by a global retrospective study (n = 110) reporting low PD-L1 expression (median 28%) and TMB (median 0.9 mut/Mb), with correspondingly poor outcomes to ICIs (median PFS 3.3 months) or chemoimmunotherapy combinations (median PFS 3.6 months)[221].
In summary, for NRG1 fusion NSCLC, EGFR/HER2-TKIs (e.g. afatinib, pyrotinib, neratinib, tarloxitinib) or HER2/HER3-targeted monoclonal antibodies/ADCs (e.g. trastuzumab, margetuximab) are recommended. If targeted therapies are unavailable, treatment strategies should follow the guidelines for stage IV NSCLC without targetable genomic alterations, as outlined in the 2024 NCCN guidelines[171].
FGFR alterations
The fibroblast growth factor receptor (FGFR) family, comprising FGFR1-4, represents a subfamily of transmembrane tyrosine kinase receptors implicated in various malignancies, including lung squamous cell carcinoma, urothelial carcinoma, and breast cancer. FGFR aberrations predominantly manifest as amplifications (most commonly FGFR1 and FGFR4), followed by mutations, rearrangements, and fusions, with FGFR1 amplifications occurring in approximately 22% of lung squamous cell carcinomas compared to only 3% of adenocarcinomas, where they may correlate with prolonged survival[222,223]. Although FGFR inhibitors (e.g., erdafitinib, pemigatinib, futibatinib, infigratinib) have demonstrated efficacy in FGFR-altered urothelial carcinoma and cholangiocarcinoma, none are currently approved for lung cancer, despite emerging signals of activity - such as pemigatinib’s promising response rates in lung cancer cohorts within pan-solid tumor trials[224]. The relationship between FGFR alterations and ICI efficacy remains controversial, with conflicting evidence across tumor types. While FGFR alterations in gastric cancer, melanoma, and NSCLC have been associated with enhanced ICI responses in some studies, others report inferior outcomes, including shorter OS in FGFR-altered melanoma and urothelial carcinoma treated with PD-1 inhibitors[225-229]. Notably, a study of 240 NSCLC patients revealed that FGFR4 alterations correlated with significantly improved ORR (50.0% vs. 19.4%; P = 0.057) and median PFS (13.17 vs. 3.17 months; P = 0.04) following PD-1/PD-L1 inhibition compared to wild-type counterparts[230]. Preclinical data suggest that combining FGFR inhibitors with ICIs may enhance antitumor immunity by increasing T-cell infiltration and inducing immunogenic cell death[231,232], though the clinical applicability of these findings requires further validation.
Given the current lack of definitive evidence supporting FGFR-directed therapies in lung cancer, the 2024 NCCN guidelines recommend managing advanced FGFR-altered NSCLC according to strategies for advanced NSCLC without targetable genomic alterations, with ongoing clinical trials expected to clarify the therapeutic potential of FGFR inhibition - either alone or in combination with immunotherapy - in this molecular subset[171].
Recommendations for immunotherapy in NSCLC with targetable genomic alterations are shown in Table 8. Clinical trials related to NSCLC are listed in Supplementary Table 1.
| First-line | Second-line and subsequent-line | |
| EGFR-sensitive mutations | Immunotherapy not recommended (Grade II recommendation). • Preferred: TKIs• Alternatives: 1. TKIs + chemotherapy2. TKIs + anti-angiogenesis 3. platinum-based chemotherapy ± bevacizumab (non-squamous)4. Amivantamab + lazertinib | Immunotherapy may be considered (Grade II recommendation)For TKI resistance with widespread progression, in the absence of effective targeted therapies • Preferred: ICI-based regimens 1. ICIs + platinum-based chemotherapy + anti-angiogenic therapy (e.g., pemetrexed + cisplatin + bevacizumab + sintilimab)2. ICIs + platinum-based chemotherapy 3. ICIs + anti-angiogenic therapy 4. Amivantamab + chemotherapy• Subsequent progression1. Single-agentchemotherapy ± bevacizumab 2. Anlotinib |
| EGFR exon 20 insertion mutation | Immunotherapy considered with caution (Grade III recommendation)• Preferred: Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations• Alternative: Amivantamab + platinum-doublet chemotherapy• If available: Sunvozertinib | Immunotherapy considered with caution (Grade III recommendation)• Preferred: Sunvozertinib• Alternatives: 1. Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations (single-agent chemotherapy or single-agent immunotherapy)2. Amivantamab |
| ALK fusion | Immunotherapy considered with caution (Grade III recommendation)• Preferred: TKIs• Alternative: platinum-based chemotherapy ± bevacizumab (non-squamous) | Immunotherapy considered with caution (Grade III recommendation)• For TKI resistance with widespread progression, in the absence of effective targeted therapies Platinum-based chemotherapy ± bevacizumab (non-squamous)• Subsequent progression: 1. Anlotinib 2. single-agent chemotherapy ± bevacizumab |
| ROS1 fusion | Immunotherapy considered with caution (Grade III recommendation)• Preferred: TKIs• Alternatives: 1. Platinum-based chemotherapy ± bevacizumab (non-squamous) 2. Repotrectinib | Immunotherapy considered with caution (Grade III recommendation)*• For TKI resistance with widespread progression, in the absence of effective targeted therapies 1. Platinum-based chemotherapy ± bevacizumab (non-squamous)2. Clinical trials 3. Repotrectinib• Subsequent progression: Single-agent chemotherapy ± bevacizumab |
| MET exon 14 skipping mutation | Immunotherapy considered with caution (Grade III recommendation) • Preferred: TKIs | Immunotherapy considered with caution (Grade III recommendation) • TKI-naïve: Preferred: TKIs• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with/without targetable genomic alterations1. Platinum-based chemotherapy ± bevacizumab (non-squamous);2. Single-agent chemotherapy ± bevacizumab; 3. Single-agent immunotherapy |
| RET fusion | Immunotherapy considered with caution (Grade III recommendation).• Preferred: Targeted therapy• Alternative: Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy considered with caution (Grade III recommendation)• TKI-naïve: 1. Preferred: Targeted therapy 2. Alternative: Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations |
| KRAS mutation | Immunotherapy may be considered except for STK11 co-mutation (Grade I recommendation)• Preferred: Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy may be considered (Grade I recommendation)• Preferred: Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• Alternative: targeted therapy- KRAS G12C inhibitors (e.g., Sotorasib, Adagrasib, Garsorasib);- KRAS G12D inhibitors (e.g., HRS-4642, MRTX-1133) |
| BRAF V600 mutation | Immunotherapy considered with caution (Grade III recommendation)• Preferred: Targeted therapy 1. Dabrafenib + trametinib 2. Encorafenib + binimetinib• Alternative:Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy considered with caution (Grade III recommendation). • TKI-naïve:1. Preferred targeted therapy 2. Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations |
| HER2 mutation | Immunotherapy considered with caution (Grade III recommendation)Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy be considered with caution (Grade III recommendation)• Preferred: Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• Alternatives: 1. Trastuzumab deruxtecan 2. Pyrotinib |
| NTRK fusion | Immunotherapy considered with caution (Grade III recommendation)• Preferred: TKIs• Alternatives: refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy be considered with caution (Grade III recommendation)• TKI-naïve: 1. Preferred: targeted therapy 2. Alternative: Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations |
| NRG1 fusion | Immunotherapy considered with caution (Grade III recommendation)Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy be considered with caution (Grade III recommendation)Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations |
| FGFR alterations | Immunotherapy considered with caution (Grade III recommendation)Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | Immunotherapy be considered with caution (Grade III recommendation)Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations |
IMMUNOTHERAPY RESISTANCE
For NSCLC patients who progress after immunotherapy, it is essential to determine the nature of resistance. In 2020, the Society for Immunotherapy of Cancer (SITC) established consensus definitions for resistance to PD-(L)1 inhibitors, categorizing it into three distinct scenarios: primary resistance, secondary resistance, and progression after treatment discontinuation. The following definitions apply to patients receiving systemic anti-PD-(L)1 monotherapy[233].
Primary resistance is defined as disease progression after at least two treatment cycles or 6 weeks of ICI therapy, with the best response being progressive disease (PD) or stable disease (SD) lasting < 6 months. A confirmatory imaging scan is required 4-12 weeks after the initial evidence of progression to rule out pseudoprogression, provided the patient is clinically stable.
Secondary resistance is defined as disease progression after ≥ 6 months of clinical benefit from ICI (CR, PR, or SD ≥ 6 months), requiring confirmatory imaging scans 4-12 weeks after the initial evidence of progression.
Progression after discontinuation is further classified based on treatment context:
(1) Adjuvant therapy resistance: Adjuvant therapy resistance is categorized based on the timing of recurrence following discontinuation of ICI treatment into primary resistance or early recurrence (progression within 12 weeks post-ICI) and late recurrence (progression > 12 weeks post-ICI). Patients who experience disease progression following adjuvant therapy should undergo biopsy to confirm the recurrence;
(2) Neoadjuvant therapy resistance: Neoadjuvant therapy resistance is categorized based on whether a MPR is achieved during neoadjuvant immunotherapy. If MPR is achieved and recurrence occurs post-surgery, it is defined as secondary resistance. Conversely, if MPR is not achieved, it is considered primary resistance. Notably, for patients receiving combined neoadjuvant and adjuvant immunotherapy, any recurrence following these treatments should be classified as adjuvant therapy resistance.
Resistance following ICI discontinuation in advanced/metastatic tumors:
(i) Primary resistance following ICI discontinuation: Primary resistance is defined as discontinuation of ICI during treatment (for toxicity or non-toxicity reasons) without evidence of prior clinical benefit (failure to achieve PR/CR before discontinuation). Patients with primary resistance are unlikely to benefit from ICI rechallenge.
(ii) Secondary resistance following ICI discontinuation: Secondary resistance is defined as disease progression occurring < 12 weeks after the last ICI dose in patients who achieved clinical benefit (PR/CR) but discontinued treatment (for toxicity or non-toxicity reasons). A confirmatory scan is recommended.
(iii) Delayed progression: Delayed progression is defined as disease progression occurring > 12 weeks after the last ICI dose in patients who achieved clinical benefit (PR/CR) but discontinued treatment (for toxicity or non-toxicity reasons). The SITC working group notes that ICI rechallenge may yield clinical benefit (> 5%) for patients with delayed progression,helping distinguish true resistance from other progression patterns.
The standardization of immunotherapy resistance definitions is crucial for guiding clinical practice and research. Table 9 presents the definitions developed by Chinese experts, which integrate the SITC’s 2020 and 2023 resistance criteria with real-world clinical practice considerations[234].
| Treatment modality | Resistance type | Drug exposure time | Best response | Re-imaging confirmation of PD | Imaging confirmation timeframe |
| ICI monotherapy or ICI-ICI combination resistance | Primary resistance | ≥ 6 weeks (2 cycles)a | PD or SD < 6 months | Yes (unless rapid tumor growth and clinical deterioration) | ≥ 4 weeks after PDb |
| Secondary resistance | ≥ 6 weeks (2 cycles) | CR, PR (no time limit) | Yes (unless rapid tumor growth and clinical deterioration) | ≥ 4 weeks after PDb | |
| ≥ 6 months | SD ≥ 6 months | ||||
| ICI-chemotherapy combination resistance | Primary resistance | ≥ 6 weeks (2 cycles)a | Any best response, < 6 months | No | / |
| Secondary resistance | ≥ 6 months | Any best response, ≥ 6 months | No | / | |
| ICI-targeted therapy combination resistance | Primary resistance | ≥ 6 weeks (2 cycles)a | PD or SD < 6 months | No | / |
| Secondary resistance | ≥ 6 weeks (2 cycles) | CR, PR (no time limit) | No | / | |
| ≥ 6 months | SD ≥ 6 months | / | / |
EVALUATION OF IMMUNOTHERAPY EFFICACY
The evaluation of immunotherapy efficacy primarily follows the Immune Response Evaluation Criteria in Solid Tumours (iRECIST)[235]. Distinct from chemotherapy, ICIs exhibit unique mechanisms of action that may lead to atypical response patterns, including delayed response, pseudoprogression (PsPD), hyperprogressive disease (HPD), and dissociated response (DR) (detailed in Table 10).
| Key parameters | Description |
| Lesion measurement | Single-dimensional measurement (details consistent with RECIST 1.1)[246] |
| Baseline target lesion Requirements (measurable lesions) | 1. Tumor lesions: Longest diameter ≥ 10 mm (CT scan with ≤ 5 mm slice thickness)2. Lymph nodes: Short axis ≥ 15 mm (CT scan with ≤ 5 mm slice thickness, consistent with RECIST 1.1) |
| Baseline target lesion quantity limit | 1. Maximum 5 target lesions total (≤ 2 per organ, consistent with RECIST 1.1)2. Lesions must be reproducibly measurable3. Measurable lesions (tumors, pathological lymph nodes, other special lesions) must be reproducible, clearly defined, easy to measure, and distant from any factors that may affect image quality |
| Non-target lesions | 1. Lesions not selected as target lesions due to the limited number of target lesions, as well as non-measurable lesions2. Involved in defining iCR and iUPD |
| New lesions | 1. Any unequivocal lesion appearing post-baseline (lesions in the same or different organs, any size) or reappearing after disappearance2. New target lesions: ≤ 5 total (≤ 2 per organ), included in SoD calculations but not baseline SoD3. New non-target lesions: All other new lesions (measurable/non-measurable) |
| iCR | Disappearance of all target/non-target lesions (normal tumor markers), lymph nodes < 10 mm, no new lesions, sustained ≥ 4 weeks |
| iPR | ≥ 30% decrease in target lesion SoD from baseline, no non-target lesion progression, no new lesions, sustained ≥ 4 weeks |
| iSD | Neither meeting iUPD nor iPR criteria (intermediate between iPR and iPD), no new lesions |
| iUPD | 1. Target lesion progression: ≥ 20% SoD increase from nadir and ≥ 5 mm absolute increase in SoD (RECIST 1.1 PD criteria)2. Non-target lesion progression: Unequivocal worsening warranting treatment discontinuation (RECIST 1.1 PD criteria)3. New lesions (RECIST 1.1 criteria)4. All iUPD requires 4-8 week confirmation. Unconfirmed cases require documentation. For confirmed iUPD, immunotherapy can be continued as long as there is no rapid tumor progression, and the patient derives clinical benefit, tolerates the treatment well, and has provided informed consent |
| iCPD | 1. Required confirmation timeframe: 4-8 weeks after initial iUPD 2. Target lesion progression: ≥ 5 mm increase in SoD from iUPD timepoint or new measurable target lesions (≥ 10 mm) 3. Non-target progression: Unequivocal worsening per RECIST 1.1 4. New lesions: Any unequivocal new lesions (measurable/non-measurable) not present at iUPD |
Delayed response
Delayed response is characterized by gradual but sustained tumor shrinkage occurring during or even after treatment discontinuation, ultimately leading to survival benefits. This pattern typically manifests as tumor response after a period of stable disease. Although standardized temporal criteria remain undefined, the median time-to-response for immunotherapy typically ranges from 2-3 months, with responses occurring beyond 12 weeks generally considered delayed. Continuation of immunotherapy is recommended in the absence of definitive progression or severe immune-related adverse events[236].
Pseudoprogression
Pseudoprogression represents a unique immunotherapy response pattern characterized by transient radiographic tumor enlargement (typically ≥ 25% increase in tumor burden) and/or emergence of new lesions during initial treatment cycles, without corresponding clinical deterioration, followed by subsequent tumor regression or stabilization confirmed through clinical or radiological and pathological assessment. This phenomenon, occurring in < 10% of cases, may result from immune-mediated inflammatory infiltration and edema rather than true neoplastic proliferation. Current evidence suggests PsPD may reflect robust immune activation within the tumor microenvironment[237-239]. When PsPD is suspected, immunotherapy continuation is only warranted when both of the following criteria are met: (1) sustained stability or improvement in tumor-related symptoms, and (2) absence of severe immune-related adverse events (irAEs). Given the relative rarity of PsPD and the potential risks of unnecessary treatment continuation, clinicians should exercise caution and obtain confirmatory evidence before maintaining immunotherapy in this clinical scenario.
Hyperprogressive disease
Currently, there is no standard definition for HPD. It is generally defined as an increase in tumor size or volume exceeding a threshold of 1.2 to 2 times within a unit of time. Some clinical studies define hyperprogression as meeting the following three criteria: (1) time to treatment failure < 2 months; (2) > 50% increase in tumor burden from baseline; (3) tumor growth rate increases by > 2 times after immunotherapy. Reported incidence ranges from 6%-29% across studies, with HPD patients demonstrating significantly worse clinical outcomes, and combining immunotherapy with chemotherapy may help prevent its occurrence[240]. When HPD is suspected, particularly in cases of clinical deterioration, immediate discontinuation of ICIs is strongly advised. Emerging evidence suggests NSCLC patients with HPD may exhibit enhanced sensitivity to salvage chemotherapy compared to historical controls[241]. For patients maintaining good performance status, prompt transition to chemotherapy or alternative therapeutic modalities is recommended.
The mechanisms underlying HPD include tumor immune microenvironment alterations, intensified innate immune suppression, activation of oncogenic signaling pathways, and dysregulation of immune-modulatory cellular components[240]. Clinical studies have identified several risk factors for HPD, including demographic characteristics such as advanced age (> 65 years), female sex, disease burden features including > 2 metastatic sites at baseline, specific molecular alterations encompassing MDM2/MDM4 amplification, EGFR/DNMT3A mutations, and 11q13 amplifications (involving CCND1, FGF3, FGF4, and FGF19)[242-245]. Despite these associations, there are no reliable biomarkers to accurately predict its occurrence, and whether HPD is unique to immunotherapy remains controversial. Therefore, in clinical practice, treatment decisions should incorporate comprehensive patient assessment (including clinical status and imaging findings), molecular profiling when available, careful risk-benefit analysis, and patient preferences, with multidisciplinary evaluation being essential to guide optimal salvage strategies upon HPD occurrence.
Dissociated response
Dissociated response is characterized by heterogeneous treatment effects across tumor lesions within individual patients, reflecting treatment efficacy and correlating with favorable prognosis. Compared to true disease progression, patients with DR exhibit prolonged OS and clinical benefit duration. Dissociated response should not be considered true progression nor acquired resistance. Immediate discontinuation of ICIs or switching to chemotherapy is not the optimal strategy. If dissociated response occurs, reassessment should be performed within 4-8 weeks, and immunotherapy should be continued.
To systematically evaluate these complex response patterns, oncologists have developed specialized immune-related response criteria including immune-related response criteria (irRC), immune-related Response Evaluation Criteria in Solid Tumors (irRECIST), immune RECIST (iRECIST), PET Response Criteria (PERCIST), and immune-modified PERCIST (imPERCIST). However, these specialized criteria remain investigational and lack formal guideline endorsement. The current iRECIST are explained in the table10 below. It is noteworthy that the widely used clinical response evaluation standard remains the classic RECIST v1.1. This is partly because the incidence of unconventional response patterns is low, with most data showing that pseudoprogression and hyperprogression rates are below 10%. Once progression occurs, it is often true progression[236].
IMMUNOTERAPY RELATED BIOMARKERS
Currently, the most widely recognized biomarkers for immunotherapy primarily include PD-L1, TMB, and MSI. With advancements in liquid biopsy technology, emerging biomarkers such as circulating tumor DNA (ctDNA), blood-based tumor mutational burden (bTMB), and gut microbiota have provided additional tools for personalized treatment strategies.
PD-L1
PD-L1 expression remains the most extensively validated biomarker for predicting patient response to PD-1/PD-L1 inhibitors. Numerous clinical studies have demonstrated a correlation between PD-L1 expression levels and the efficacy of ICIs. Currently, pembrolizumab and atezolizumab monotherapies are approved for first-line treatment of advanced metastatic NSCLC with high PD-L1 expression. The IMpower110 trial revealed that patients with EGFR/ALK wild-type advanced NSCLC and high PD-L1 expression (TC ≥ 50% or IC ≥ 10%) derived significant survival benefits from atezolizumab monotherapy. Similarly, the KEYNOTE-024 study demonstrated improved outcomes in EGFR/ALK wild-type advanced NSCLC patients with PD-L1 ≥ 50% treated with pembrolizumab[67,69].
However, the predictive value of PD-L1 is not absolute, as approximately 10% of patients with negative PD-L1 expression may still respond to immunotherapy. Studies such as ORIENT-12, KEYNOTE-407 and KEYNOTE-189 demonstrated that even PD-L1-negative patients can benefit from immunotherapy[72,80,112]. This phenomenon may be related to the tumor heterogeneity of PD-L1 expression, variations in PD-L1 detection methods, and the dynamic changes in PD-L1 expression. Future research should focus on optimizing PD-L1 detection techniques to improve standardization and reproducibility of results. Additionally, we can develop integrated predictive models combining PD-L1 with complementary biomarkers like TMB and TME characteristics for comprehensive therapeutic guidance.
Tumor mutational burden
TMB is another important biomarker for evaluating the efficacy of ICI.s It is defined as the number of somatic non-synonymous mutations within the tumor genome, typically expressed as mutations per megabase (mut/Mb). Higher TMB is thought to correlate with increased neoantigen production, which may enhance the patient’s response to ICI. The KEYNOTE-158 study demonstrated that patients with high TMB (≥ 10 mut/Mb) achieved an ORR of 29% with pembrolizumab, compared to only 6% in those with low TMB (< 10 mut/Mb)[247]. Based on these findings, the FDA approved pembrolizumab In June 2020 for advanced solid tumor with high TMB (TMB-H ≥ 10 mut/Mb) that progressed on prior therapies, with FoundationOne CDx as the companion diagnostic assay.
A retrospective exploratory analysis of the KEYNOTE-042 study showed that among PD-L1 TPS ≥ 1% advanced NSCLC patients treated with pembrolizumab monotherapy, higher tTMB (≥ 175 mut/exome) was associated with better clinical outcomes (HR for OS: 0.62 [0.48-0.80] vs. 1.09 [95% CI 0.88-1.36])[248]. Similarly, The CheckMate-159 study and research by Forde et al.[18] and Ricciutiet al.[249] also demonstrated that patients with high TMB can benefit from immunotherapy.
Despite these promising findings, the role of TMB as an independent predictive biomarker remains controversial. Although initial results of the CheckMate-227 trial suggested that high TMB could predict the efficacy of nivolumab plus ipilimumab, studies such as KEYNOTE-021, KEYNOTE-189, and KEYNOTE-407 found no significant correlation between TMB and the efficacy of pembrolizumab plus chemotherapy, indicating that patients with low TMB may still respond to immunotherapy, while those with high TMB do not always benefit[250].
Several technical and methodological challenges hinder the widespread adoption of TMB in clinical practice. These include variability in sequencing platforms and the lack of standardized cutoff values. For instance, discrepancies in panel size, gene coverage, and mutation calling algorithms can lead to inconsistent TMB quantification across studies. To address these issues, future efforts should focus on harmonizing TMB measurement methodologies, validating its predictive utility in prospective trials, and integrating TMB with complementary biomarkers to refine patient selection for immunotherapy. Until then, clinical decision-making should consider TMB alongside other relevant factors rather than relying on it as a standalone predictor.
Microsatellite instability
The DNA mismatch repair (MMR) system plays a critical role in maintaining genomic stability by correcting errors during DNA replication and recombination. Dysfunction in this system leads to defective mismatch repair (dMMR), resulting in the accumulation of somatic mutations and microsatellite instability (MSI). High-frequency MSI (MSI-H) represents the phenotypic manifestation of dMMR and has been established as a predictive biomarker for ICI efficacy in certain cancers, particularly colorectal and endometrial carcinomas[251].
While MSI-H/dMMR is relatively rare in NSCLC, occurring in approximately 1% of cases, emerging evidence suggests its potential role in predicting immunotherapy response[252]. MSI-H NSCLC tumors often exhibit elevated TMB and increased TILs, including activated CD4+ memory T cells and CD8+ cytotoxic T cells[253]. Furthermore, mutations in MMR genes (e.g., MLH1, MSH2, MSH6, and PMS2) have been associated with improved responses to ICIs such as nivolumab[254,255]. In 2017, the FDA approved the pembrolizumab for the treatment of all advanced solid tumor with MSI-H/dMMR, marking the first approval based on biomarker data[256]. This decision highlights the significant clinical potential of MSI in immunotherapy.
Despite promising findings, research on MSI-H/dMMR in NSCLC remains limited. Further studies are needed to validate its predictive role and explore potential synergies with other biomarkers, such as PD-L1 and TMB. Standardized testing methodologies and prospective clinical trials will be essential to refine patient selection and optimize immunotherapy strategies for this subset of NSCLC patients.
Tumor infiltrating lymphocytes
TILs are crucial predictive biomarkers in NSCLC immunotherapy, composed of heterogeneous immune cells (T cells, B cells, NK cells) that infiltrate tumors to mediate anti-tumor immunity. PD-L1 expression correlates with intratumoral CD8+ T-cell density, and TIL infiltration levels predict both ICI efficacy and TME immunogenicity. studies have shown that the abundance of TILs is significantly associated with PFS and OS in NSCLC[257,258]. In nivolumab-treated NSCLC, high-TIL patients showed median PFS of 13 vs. 2.2 months in low-TIL groups, with median OS not reach (NR) vs. 8.4 months[258].
Tumor-infiltrating lymphocytes (TILs) have emerged as crucial predictive biomarkers for immunotherapy response in NSCLC. These heterogeneous immune cell populations, comprising T cells, B cells, and natural killer cells, infiltrate tumor tissues and play a pivotal role in mediating anti-tumor immunity. The clinical significance of TILs is underscored by their correlation with patient outcomes, where TIL infiltration levels can predict both ICI efficacy and TME immunogenicity and studies have shown that the abundance of TILs is significantly associated with PFS and OS in NSCLC[257,258]. In nivolumab-treated NSCLC cohorts, patients with high TIL infiltration achieved significantly PFS (13 vs. 2.2 months) and OS (NR vs. 8.4 months) compared to those with low TIL levels.
Additionally, CD8+ T-cell density frequently correlates with PD-L1 positivity. Based on the status of PD-L1 and TILs, the TME in NSCLC can be classified into four types: Type I (PD-L1+, TIL+), Type II (PD-L1-, TIL-), Type III (PD-L1+, TIL-), and Type IV (PD-L1-, TIL+), with Type I showing optimal response to ICIs and Type IV exhibiting poor monotherapy outcomes[259-262]. Notably, high level of CD8+ T cells is crucial for the efficacy of anti-PD-1/PD-L1 treatment. However, despite the significant potential of TILs in immunotherapy, challenges remain in their detection methods and standardization, necessitating further research to optimize their application.
Others
The indicators mentioned above are mostly obtained from tumor tissue. Recently, liquid biopsy technology has rapidly advanced. Compared to traditional tissue biopsy, liquid biopsies offer distinct advantages including minimal invasiveness, repeatability, and improved patient tolerance. ctDNA has emerged as a particularly valuable tool, demonstrating utility in early cancer detection, treatment response monitoring, and recurrence prediction.
The CheckMate-816 study revealed that ctDNA clearance following neoadjuvant therapy correlated with higher pCR rates and improved EFS. Notably, postoperative ctDNA positivity may indicate minimal residual disease and increased recurrence risk, providing critical prognostic information[27].
bTMB is another important circulating tumor biomarker, with IMpower110 study demonstrating that bTMB can serve as an independent biomarker. Retrospective analyses of the POPLAR and OAK studies showed good consistency between bTMB and tissue-based TMB (tTMB), with bTMB ≥ 16 mut/Mb NSCLC patients experiencing longer PFS when treated with atezolizumab as second-line therapy[65]. The phase II B-F1RST trial further validated this conclusion[263]. Beyond these, emerging peripheral blood markers including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lactate dehydrogenase (LDH), interferon (IFN) signatures, and T cell receptor (TCR) repertoire analysis are being investigated for their potential in immunotherapy response prediction.
In addition, comprehensive genomic profiling has revealed significant associations between specific mutations and immunotherapy outcomes. The IMMUNOTARGET study showed that NSCLC patients with targetable genomic alterations had poor efficacy when treated with ICI monotherapy, with an ORR of 0% in ALK fusion-positive patients, indicating no benefit from immunotherapy[172]. Clinically, EGFR mutations, ALK fusions, ROS1 fusions, and RET fusions are often associated with low tumor immunogenicity and non-inflammatory TME, resulting in limited benefit from immunotherapy. In contrast, KRAS mutations and TP53 mutations are associated with high tumor immunogenicity and an inflammatory TME, making immunotherapy a viable option in the absence of targeted therapies. Furthermore, mutations in DNA polymerase epsilon and DNA polymerase delta 1 are positive indicators for immunotherapy, while STK11 mutations and KEAP1 mutations are negative markers for immunotherapy.
What’s more, gut microbiota has also become a hotspot in immunotherapy research recently. Studies have found that the use of antibiotics and proton pump inhibitors during immunotherapy significantly shortens OS in NSCLC patients[264]. Recent research has identified the gut microbiota as a novel modulator of immunotherapy response. Clinical observations reveal that antibiotic use during immunotherapy significantly reduces overall survival in NSCLC patients. Stusy by Routy et al. (2018) demonstrated that immunotherapy responders harbor more diverse gut microbiomes, with particular enrichment of Akkermansia muciniphila and Enterococcus species. These patients exhibited enhanced memory T cell responses against these bacteria, suggesting a mechanistic link between microbiome composition and anti-tumor immunity. Subsequent studies revealed that fecal microbiota transplantation or supplementation with Akkermansia muciniphila could overcome antibiotic-associated immunotherapy resistance[265]. While these findings position the gut microbiome as a potential predictive biomarker, current technological limitations in microbial profiling and incomplete understanding of underlying mechanisms necessitate further investigation. Future research should focus on standardizing microbiome analysis methods and elucidating the precise immunological interactions between gut microbes and anti-tumor immunity.
ADVERSE REACTIONS AND MANAGEMENT OF IMMUNOTHERAPY
The mechanisms underlying ICI-related toxicities are not fully understood and may involve genetic factors, disruption of immune tolerance, cross-reactive antigen responses, production of cytokines/chemokines, off-target effects, and the influence of the microbiome[266,267].
irAEs are characterized by diversity, specificity, and temporal dynamics. The diversity is reflected in the fact that irAEs can occur in any organ, with the gastrointestinal tract, liver, skin, and endocrine organs being the most commonly affected, while cardiovascular and neurologic toxicities are relatively rare. The specificity is demonstrated by the distinct toxicity profiles of different ICIs, with PD-1 inhibitors more likely to cause pneumonitis, myalgia, thyroiditis, arthritis, and vitiligo, and CTLA-4 inhibitors more prone to colitis, hypophysitis, and rash[268]. Meanwhile, different PD-1/PD-L1 inhibitors also have varying toxicity profiles, with nivolumab more commonly causing endocrine toxicities, pembrolizumab more frequently associated with arthritis, pneumonitis, and hepatotoxicity, while the PD-L1 inhibitor atezolizumab is more likely to induce hypothyroidism, nausea, and vomiting, and camrelizumab is prone to causing reactive cutaneous capillary endothelial proliferation[269]. Additionally, the same ICIs used for different cancers can produce different toxicity profiles. For example, in melanoma, PD-1 inhibitors are more likely to induce gastrointestinal and cutaneous toxicities, whereas in lung cancer, pneumonitis is more prevalent, and in renal cancer, pneumonitis and dyspnea are common[269]. Regarding temporal dynamics, irAEs can occur at any time following treatment initiation, usually within 1-6 months, with gastrointestinal and cutaneous toxicities often emerging first[270]. Importantly, irAEs can still occur even after discontinuation of ICIs. Therefore, clinicians must remain vigilant and continuously assess and monitor for AE at any time.
Overall, ICIs demonstrate a favorable safety profile, with the incidence of all-grade irAEs being approximately 66%, and the incidence of grade ≥ 3 irAEs being around 14%. Toxicity frequencies follow a hierarchical pattern: PD-1 inhibitors exhibit higher irAE rates than PD-L1 agents, while CTLA-4 inhibitors surpass PD-1/PD-L1 inhibitors, and combination therapies incur the greatest toxicity rates[271,272]. Specifically, the median incidence of overall toxicity for CTLA-4 inhibitors, PD-1 inhibitors, PD-L1 inhibitors, and PD-1/PD-L1 plus CTLA-4 inhibitors are 90.5%, 75.7%, 66.6% and 94.2%, respectively. The corresponding median incidence rates of grade ≥ 3 toxicity are 38.8%, 17.6%, 15.7%, and 57.7%, respectively. Compared to PD-1/PD-L1 inhibitors, CTLA-4 inhibitors are associated with a higher incidence of AEs, which may be related to their roles in different stages of the immune response. CTLA-4 primarily functions during the initial immune activation phase in lymphoid organs, where its blockade promotes broad T-cell repertoire expansion and enhances activation of naïve T cells - effects that may explain its more extensive toxicity profile. In contrast, PD-1/PD-L1 interactions primarily modulate effector-phase immunity in peripheral tissues, with inhibition selectively enhancing already-primed, tumor-specific T-cell responses while theoretically preserving broader immune homeostasis.
Although ICIs generally have a favorable safety profile, a small proportion of patients may experience fatal toxicities, with mortality rates of 1.08% for CTLA-4 inhibitors, 0.36% for PD-1 inhibitors, and 0.38% for PD-L1 inhibitors. The median time to fatal irAEs is 40 days for these agents. When PD-1/PD-L1 inhibitors are combined with CTLA-4 inhibitors, the mortality rate increases to 1.23%, and the median time to fatal irAEs shortens to 14 days[272]. Additionally, cardiac toxicities such as myocarditis, although rare (0.06% with nivolumab monotherapy; 0.27% with nivolumab plus ipilimumab), can result in a mortality rate as high as 50% if they manifest. Therefore, it is crucial to remain vigilant in recognizing AEs promptly and intervening in a timely manner.
The management of irAEs follows a graded approach based on CTCAE criteria, with treatment decisions balancing immunosuppressive needs against cancer therapy continuation. For Grade 1 toxicities, ICIs may typically continue or temporarily pause alongside symptomatic management and close monitoring. Grade 2 events generally require temporary ICI interruption and consideration of low-to-moderate dose corticosteroids, with notable exceptions including hemolytic anemia and Guillain-Barré syndrome which mandate permanent discontinuation even at this grade. Severe Grade 3/4 toxicities necessitate immediate high-dose corticosteroids and permanent ICI cessation in most cases, though endocrine disorders often permit treatment continuation after appropriate hormone replacement.
Based on the mechanisms of irAEs, most non-endocrine irAEs require immunosuppressive therapy. Immunosuppressants can be categorized into four classes: corticosteroids, cytotoxic agents, calcineurin inhibitors, and biologics. These drugs inhibit cellular and humoral immunity from different perspectives, particularly in suppressing T cells. Corticosteroids are the therapeutic backbone, controlling the majority of irAEs. If corticosteroids are effective, they should be tapered over 4-6 weeks to the minimal effective dose. For the rare patients who cannot completely discontinue corticosteroids, ICI therapy can be restarted as long as the daily dose of prednisone is ≤ 10 mg (or equivalent) and no other immunosuppressants are being used concurrently. For severe irAEs, if there is no significant improvement after 2-3 days of corticosteroid therapy, early combination with other immunosuppressants, such as mycophenolate mofetil, infliximab, or anti-thymocyte globulin, should be considered. Additionally, attention must be paid to the adverse effects of these drugs. Long-term corticosteroid use requires prophylaxis against hyperglycemia, gastritis, opportunistic bacterial or fungal infections, and osteoporosis. Patients receiving immunosuppressants should also be monitored for the risk of hepatitis B/C virus reactivation and tuberculosis. Moreover, multidisciplinary consultation and collaboration with relevant specialists are essential to develop experience in the diagnosis and treatment of irAEs.
In summary, optimal management of irAEs necessitates a systematic five-component approach: prevention, anticipation, diagnosis, treatment, and monitoring. Prevention requires clinician familiarity with irAE profiles and comprehensive patient education about potential toxicities. Anticipation involves baseline assessments before treatment initiation and regular monitoring for early detection. Diagnosis mandates thorough evaluation of new or worsening symptoms post-ICI administration, often requiring multidisciplinary input to confirm irAEs and determine severity. Treatment follows grade-adapted algorithms to balance immunosuppression with cancer therapy continuation. Monitoring should extend for ≥ 1 year post-treatment to detect late-onset irAEs and manage treatment-related complications, particularly steroid-induced adverse effects.
SUMMARY AND PROSPECT
Our expert group established 15 consensus statements and recommendations regarding the use of immune checkpoint inhibitors for NSCLC [Tables 11 and 12], as well as a recommended treatment algorithm [Figures 1 and 2]. The application of ICIs in NSCLC has evolved from monotherapy to various combination strategies, including integration with chemotherapy, radiotherapy, and anti-angiogenic therapy. Substantial clinical trial evidence has demonstrated the efficacy and safety of these combinatorial approaches, leading to corresponding updates in treatment guidelines. Nevertheless, challenges persist in optimizing immunotherapy implementation. These include the effective management of immune-related toxicities, refinement of predictive biomarkers for patient stratification, and determination of optimal combination strategies with appropriate treatment timing. Future progress will require continued efforts to develop biomarker-driven approaches and personalized treatment paradigms to maximize survival outcomes while preserving quality of life for NSCLC patients.
Figure 1.The treatment process for stage I-III NSCLC. 1. Management of Incomplete Resection: Stage I/II: Reoperation or re-irradiation may be considered, with adjuvant therapy strongly recommended for stage II and optional for stage I. Stage III: Concurrent chemoradiotherapy followed by adjuvant therapy is preferred. 2. MDT discussion is strongly advised for optimal treatment planning, particularly for stage III disease. 3. aIf the patient is not suitable for surgery or refuses surgery, definitive radiotherapy may be considered. bPreferred for Pancoast Tumors. cHigh-risk factors: Poorly differentiated tumors (excluding well-differentiated neuroendocrine tumors, but including other neuroendocrine tumors), lymphovascular invasion, visceral pleural invasion, air-space spread, palliative resection, and predominant pathological subtypes such as solid or micropapillary patterns. dIf ICIs were used in the neoadjuvant setting, it is recommended to use the same ICIs in the adjuvant setting. MDT: Multidisciplinary team; PD: progressive disease; non-PD: non-progressive disease; EGFR: epidermal growth factor receptor; PD-L1: programmed death-ligand 1; TKI: tyrosine kinase inhibitor; NSCLC: non-small cell lung cancer; ICI: immune checkpoint inhibitor.
Figure 2.The treatment process for stage IV NSCLC. 1. Anti-angiogenic therapy is not recommended for squamous cell carcinoma NSCLC. 2. aThe medical evidence is insufficient. Clinicians may consider immunotherapy based on the patient’s physical condition, disease status, and preferences. PD-L1: Programmed death-ligand 1; MDT: multidisciplinary team; EGFR: epidermal growth factor receptor; KRAS: Kirsten rat sarcoma viral oncogene homolog; STK11: serine/threonine kinase 11; ALK: anaplastic lymphoma kinase; ROS1: ROS proto-oncogene 1; RET: rearranged during transfection; MET: mesenchymal-epithelial transition factor; BRAF V600: BRAF proto-oncogene, V600E mutation; NTRK: neurotrophic tyrosine receptor kinase; HER2: human epidermal growth factor receptor 2; NRG1: neuregulin 1; FGFR: fibroblast growth factor receptor; ICI: immune checkpoint inhibitor; ADC: antibody-drug conjugate; NSCLC: non-small cell lung cancer.
| Item | Consensus | Descriptions | Recommendation level |
| Timing of testing | Consensus 1 | PD-L1, TMB, and MSI should be tested at initial diagnosis and prior to any treatment regimen changes | Grade I recommendation |
| Consensus 2 | PD-L1, TMB, and MSI should be tested for stage II and stage III NSCLC after operation to guide adjuvant immunotherapy | Grade I recommendation | |
| Consensus 3 | PD-L1, TMB, and MSI should be tested in unresectable stage III and stage IV NSCLC before treatment | Grade I recommendation | |
| Consensus 4 | PD-L1, TMB, and MSI should be tested when considering ICIs as subsequent-line therapy or ICIs plus chemotherapy as first-line treatment | Grade II recommendation | |
| Consensus 5 | PD-L1 testing should be performed concurrently for patients with targetable genomic alterations | Grade II recommendation | |
| Testing methods | Consensus 6 | Immunohistochemistry for PD-L1 testing;Next-generation sequencing for TMB and MSI testing | Grade I recommendation |
| Consensus 7 | Use Formalin-fixed paraffin-embedded tumor tissue for testing;Do not use blood samples for PD-L1 testing | Grade I recommendation | |
| Consensus 8 | Testing should be performed on both primary and metastatic lesions when necessary. | Grade I recommendation | |
| Consensus 9 | Testing should focus on tumor region that best represents disease progression or in the area with the poorest differentiation. | Grade II recommendation | |
| Consensus 10 | Testing should be performed on multiple biopsy blocks or specimens, with focus on the highest TPS/TC value. | Grade II recommendation | |
| Consensus 11 | Testing can be performed on cytological specimens. | Grade II recommendation | |
| Testing quality control | Consensus 12 | All tests should be performed in accredited laboratories (such as ISO15189, CAP, or CLIA) with proper quality control for PD-L1, TMB, and MSI analysis. | Grade I recommendation |
| Consensus 13 | Companion diagnostic antibodies should match the specific PD-1/PD-L1 inhibitors, using the corresponding antibody clones, testing platforms, and interpretation criteria (see Tables 2 and 3 for details). | Grade I recommendation | |
| Consensus 14 | Standardize pre-analytical variables: specimen type, cold ischemia time, fixation protocol, slide preparation, and storage conditions. | Grade I recommendation | |
| Treatment recommendation | Consensus 15 | See Table 12 below for detailed treatment recommendations | / |
| Grade I recommendation | Grade II recommendation | Grade III recommendation | |
| Resectable NSCLC | 1. Adjuvant atezolizumab after radical surgery(IMpower010) (Stage II-IIIA, PD-L1 ≥ 1%)a2. Neoadjuvant nivolumab plus platinum-based chemotherapy (CheckMate-816) (Tumor ≥ 4 cm or lymph node involvement)a3. Perioperative toripalimab plus platinum-based chemotherapy followed by adjuvant toripalimab maintenance(NEOTORCH) (Stage IIIA-IIIB)a | 1. Adjuvant pembrolizumab after radical surgery (KEYNOTE-091) (IB [T ≥ 4 cm] - IIIA)a2. Neoadjuvant pembrolizumab plus platinum-based chemotherapy, followed by adjuvant pembrolizumab (KEYNOTE-671) (Stage II-IIIB [N2])a3. Neoadjuvant tislelizumab plus platinum-based chemotherapy, followed by adjuvant tislelizumab (RATIONALE-315) (Stage II-IIIA)a | 1. Neoadjuvant nivolumab plus platinum-based chemotherapy, followed by adjuvant nivolumab (CheckMate-77T) (Stage II-IIIB)a2. Neoadjuvant durvalumab plus platinum-based chemotherapy, followed by adjuvant durvalumab (AEGEAN) (Stage IIA-IIIB [N2])a |
| Unresectable locally advanced NSCLC | |||
| PS = 0-1 | 1. Durvalumab consolidation for patients without progression after definitive concurrent chemoradiotherapy (PACIFIC)2. Sugemalimab consolidation for patients without progression after concurrent or sequential chemoradiotherapy (GEMSTONE-301) | Sequential chemoradiotherapy | / |
| PS = 2 | Radiotherapy alone or sequential chemoradiotherapy | 1. Chemotherapy alone2. Targeted therapy | / |
| Stage IV Squamous NSCLC without targetable genomic alterations | |||
| First-line PS = 0-1 | 1. Atezolizumab (limited to TPS ≥ 50% or IPS ≥ 10%) (IMPOWER110) 2. Pembrolizumab (TPS ≥ 50%, PD-L1 TPS 1%-49%) (KEYNOTE-024、KEYNOTE-042) 3. Paclitaxel/nab-paclitaxel + platinum+ pembrolizumab (KEYNOTE-407) or tislelizumab (RATIONALE-307) 4. Paclitaxel + platinum + camrelizumab (CameL-sq) or sugemalimab (GEMSTONE-302) or penpulimab (AK105-302) 5. Gemcitabine + platinum + sintilimab (ORIENT-12) 6.Nab-paclitaxel + platinum + serplulimab (ASTRUM-004) | 1. Cemiplimab (PD-L1 TPS ≥ 50%) (EMPOWER-Lung 1) 2. Paclitaxel + platinum + cemiplimab (EMPOWER-Lung 3) | 1.Nivolumab + ipilimumab + 2 cycles paclitaxel-platinum (CheckMate-9LA) 2. Durvalumab + tremelimumab + gemcitabine/paclitaxel/nab-paclitaxel + platinum (POSEIDON) |
| First-line PS=2 | Atezolizumab monotherapy (IPSOS) | / | / |
| Second-line | 1.MDT consultation 2.Participation in clinical trials3.For prior PD-1/L1 inhibitor use: Chemotherapy (± antiangiogenic therapy).No prior PD-1/L1 inhibitor use: 1)Nivolumab (CheckMate-078) 2) Tislelizumab (RATIONALE-303) | No prior PD-1/L1 inhibitor use: 1) Pembrolizumab (limited to PD-L1 TPS > 1%) (KEYNOTE-010) 2) Atezolizumab (OAK) | For oligoprogression: Consider ICIs + local therapy (radiotherapy/ablation) |
| Third-line | 1.MDT consultation 2.Participation in clinical trials.3.For no prior PD-1/L1 inhibitor use: Nivolumab(CheckMate-078) | / | / |
| Stage IV Non-squamous NSCLC without targetable genomic alterations | |||
| First-line PS = 0-1 | 1. Atezolizumab (TC ≥ 50% or IC ≥ 10%) (IMpower110)2. Pembrolizumab (limited to TPS ≥ 50%, TPS 1%-49%) (KEYNOTE-024, KEYNOTE-042) 3. Pemetrexed + platinum + Camrelizumab (CAMEL) or Sintilimab (ORIENT-11) or Tislelizumab (RATIONALE-304) or Atezolizumab (IMpower132) or Sugemalimab (GEMSTONE-302) or Toripalimab (CHOICE-01) | 1. Paclitaxel + carboplatin + bevacizumab + atezolizumab (IMpower150) 2. Nab-paclitaxel + carboplatin + atezolizumab (IMpower130) 3. Cemiplimab (PD-L1 TPS ≥ 50%) (EMPOWER-Lung 1) 4. Pemetrexed/paclitaxel + platinum + cemiplimab (EMPOWER-Lung 3) | 1. Nivolumab + ipilimumab+ 2 cycles paclitaxel/platinum (CheckMate-9LA) 2. Durvalumab + tremelimumab + gemcitabine/paclitaxel/nab-paclitaxel + platinum (POSEIDON) |
| First-linePS = 2 | / | Atezolizumab (IPSOS) | / |
| Second-line | 1. MDT consultation 2. Participation in clinical trials3. For prior PD-1/L1 inhibitor use: Chemotherapy (± antiangiogenic therapy).No prior PD-1/L1 inhibitor use:1) Nivolumab (CheckMate-078)2) Tislelizumab (RATIONALE-303) | No prior PD-1/L1 inhibitor use: 1) Pembrolizumab (TPS > 1%) (KEYNOTE-010) 2) Atezolizumab (OAK) | For oligoprogression: Consider ICIs + local therapy (RT/ablation) |
| Third-Line | 1. MDT consultation 2. Participation in clinical trials3. No prior PD-1/L1 inhibitor use:1) Nivolumab (CheckMate-078)2) Tislelizumab (RATIONALE-303) | / | / |
| Stage IV NSCLC with targetable genomic alterations | |||
| EGFR sensitive mutations | First-line treatment:Immunotherapy not recommended (Grade II recommendation)• Preferred: TKIs• Alternatives: 1. TKIs + chemotherapy2. TKIs + anti-angiogenesis 3. platinum-based chemotherapy ± bevacizumab (non-squamous)4. Amivantamab + lazertinib | ||
| Second-line and subsequent-line treatment:Immunotherapy may be considered (Grade II recommendation)For TKI resistance with widespread progression, in the absence of effective targeted therapies • Preferred: ICI-based regimens 1. ICIs + platinum-based chemotherapy + anti-angiogenic therapy (e.g., pemetrexed + cisplatin + bevacizumab + sintilimab)2. ICIs + platinum-based chemotherapy3. ICIs + anti-angiogenic therapy4. Amivantamab + chemotherapy• Subsequent progressionSingle-agent chemotherapy ± bevacizumab Anlotinib | |||
| ALKfusion | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).• Preferred: TKIs• Alternative: platinum-based chemotherapy ± bevacizumab (non-squamous) | ||
| Second-line and subsequent-line treatment:Immunotherapy considered with caution (Grade III recommendation)• For TKI resistance with widespread progression, in the absence of effective targeted therapies Platinum-based chemotherapy ± bevacizumab (non-squamous)• Subsequent progression: 1. Anlotinib 2. single-agent chemotherapy ± bevacizumab | |||
| ROS1 fusion | First-line treatment:Immunotherapy considered with caution (Grade III recommendation)• Preferred: TKIs• Alternatives: 1. Platinum-based chemotherapy ± bevacizumab (non-squamous) 2. Repotrectinib | ||
| Second-line and Subsequent-line Treatment:Immunotherapy considered with caution (Grade III recommendation)• For TKI resistance with widespread progression, in the absence of effective targeted therapies Platinum-based chemotherapy ± bevacizumab (non-squamous)Clinical trials Repotrectinib• Subsequent progression: Single-agent chemotherapy ± bevacizumab | |||
| RET fusion | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).• Preferred: targeted therapy• Alternative: refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | ||
| Second-line and subsequent-line treatment:Immunotherapy considered with caution (Grade III recommendation).• TKI-naïve: Preferred: targeted therapy Alternative: refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations (platinum-based chemotherapy ± bevacizumab) | |||
| MET exon 14 skipping mutation | First-line treatment:Immunotherapy considered with caution (Grade III recommendation) • Preferred: TKIs | ||
| Second-line and subsequent-line treatment:Immunotherapy considered with caution (Grade III recommendation).• TKI-naïve: Preferred: TKIs• TKI-treated: refer to the treatment strategy for stage IV NSCLC with/without targetable genomic alterations1. Platinum-based chemotherapy ± bevacizumab (non-squamous); 2. Single-agent chemotherapy ± bevacizumab; 3. Single-agent immunotherapy | |||
| EGFR exon 20 insertion mutation | First-line treatment:Immunotherapy considered with caution (Grade III recommendation)• Preferred: Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations• Alternative: Amivantamab + platinum-doublet chemotherapy• If available: Sunvozertinib | ||
| Second-line and subsequent-line treatment:Immunotherapy considered with caution (Grade III recommendation).Immunotherapy considered with caution (Grade III recommendation).• Preferred: Sunvozertinib• Alternatives: 1. Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations (single-agent chemotherapy or single-agent immunotherapy)2. Amivantamab | |||
| BRAF V600 mutation | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).• Preferred: Targeted therapy 1. Dabrafenib + trametinib 2. Encorafenib + binimetinib• AlternativeRefer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | ||
| Second-line and subsequent-line treatment:Immunotherapy considered with caution (Grade III recommendation)• TKI-naïve:Preferred targeted therapy Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations | |||
| NTRK Fusion | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).• Preferred: TKIs• Alternatives: Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | ||
| Second-line and subsequent-line treatment:Immunotherapy be considered with caution (Grade III recommendation). • TKI-naïve: 1. Preferred: targeted therapy 2. Alternative: Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• TKI-treated: Refer to the treatment strategy for stage IV NSCLC with targetable genomic alterations | |||
| KRAS GI2C Mutation | First-Line Treatment:Immunotherapy may be considered except for STK11 co-mutation (Grade I recommendation)• Preferred: refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations (Patients with KRAS/TP53 co-mutations benefit more from immunotherapy, while those with KRAS/STK11 co-mutations benefit less) | ||
| Second-line and subsequent-line treatment:Immunotherapy may be considered (Grade I recommendation)• Preferred: refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations• Alternative: targeted therapy- KRAS G12C inhibitors (e.g., Sotorasib, Adagrasib, Garsorasib).- KRAS G12D inhibitors (e.g., HRS-4642, MRTX-1133). | |||
| HER2 Mutation | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations. | ||
| Second-line and subsequent-line treatment:Immunotherapy be considered with caution (Grade III recommendation). • Preferred: refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations.• Alternatives: 1. Trastuzumab deruxtecan 2. Pyrotinib | |||
| NRG1 fusion | First-line treatment:Immunotherapy considered with caution (Grade III recommendation).Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | ||
| Second-line and Subsequent-line Treatment:Immunotherapy be considered with caution (Grade III recommendation)Refer to the treatment strategy for stage IV NSCLC without targetable genomic alteration | |||
| FGFR alterations | First-line treatment:Immunotherapy be considered with caution (Grade III recommendation). Refer to the first-line treatment strategy for stage IV NSCLC without targetable genomic alterations | ||
| Second-line and subsequent-line treatment:Immunotherapy be considered with caution (Grade III recommendation)Refer to the treatment strategy for stage IV NSCLC without targetable genomic alterations | |||
References
- Sung H, Ferlay J, Siegel RL. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin.. 2021; 71:209-49. DOI
- Han B, Zheng R, Zeng H. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent.. 2024; 4:47-53. DOI | PubMed |
- Rosell R, Karachaliou N. Large-scale screening for somatic mutations in lung cancer. Lancet.. 2016; 387:1354-6. DOI
- Wozniak AJ, Gadgeel SM. Review: Adjuvant therapy for resected non-small cell lung cancer. Ther Adv Med Oncol.. 2009; 1:109-18. DOI | PubMed |
- Goldstraw P, Chansky K, Crowley J. The IASLC Lung Cancer Staging Project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J Thorac Oncol.. 2016; 11:39-51. DOI
- Xu C, Hao Y, Wang D. ECLUNG consensus/guidelines development principles and methods (2024 edition). Intell Pharm.. 2025; 3:141-2. DOI
- Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity.. 2013; 39:1-10. DOI
- Baumeister SH, Freeman GJ, Dranoff G, Sharpe AH. Coinhibitory pathways in immunotherapy for cancer. Annu Rev Immunol.. 2016; 34:539-73. DOI
- Andrews LP, Marciscano AE, Drake CG, Vignali DAA. LAG3 (CD223) as a cancer immunotherapy target. Immunol Rev.. 2017; 276:80-96. DOI | PubMed |
- Das M, Zhu C, Kuchroo VK. Tim‐3 and its role in regulating anti‐tumor immunity. Immunol Rev.. 2017; 276:97-111. DOI | PubMed |
- Sakuishi K, Apetoh L, Sullivan JM, Blazar BR, Kuchroo VK, Anderson AC. Targeting Tim-3 and PD-1 pathways to reverse T cell exhaustion and restore anti-tumor immunity. J Exp Med.. 2010; 207:2187-94. DOI | PubMed |
- Yu X, Harden K, C Gonzalez L. The surface protein TIGIT suppresses T cell activation by promoting the generation of mature immunoregulatory dendritic cells. Nat Immunol.. 2008; 10:48-57. DOI
- Johnston RJ, Comps-agrar L, Hackney J. The immunoreceptor TIGIT regulates antitumor and antiviral CD8+ T cell effector function. Cancer Cell.. 2014; 26:923-37. DOI
- Lung Cancer Study Group and Molecular Pathology Collaboration Group of Tumor Pathology Committee of Chinese Anti-Cancer Association; Lung Cancer Professional Committee of Chinese Anti-Cancer Association; Expert Committee on Non-Small Cell Lung Cancer of Chinese Society of Clinical Oncology. [Chinese expert consensus on clinical testing standards of PD-L1 expression for non-small cell lung cancer (2023 version)]. Zhonghua Bing Li Xue Za Zhi.. 2024; 53:121-9. DOI
- Pathology Quality Control Center; Chinese Society of Pathology; Pathology Committee of Chinese Society of Clinical Oncology. [Consensus on the immunohistochemical tests of PD-L1 in solid tumors (2021 version)]. Zhonghua Bing Li Xue Za Zhi.. 2021; 50(7):710-8. DOI
- Jørgensen JT. Companion and complementary diagnostics: clinical and regulatory perspectives. Trends in Cancer.. 2016; 2:706-12. DOI
- Teixidó C, Vilariño N, Reyes R, Reguart N. PD-L1 expression testing in non-small cell lung cancer. Ther Adv Med Oncol.. 2018; 10:1758835918763493. DOI | PubMed |
- Forde PM, Chaft JE, Smith KN. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med.. 2018; 378:1976-86. DOI
- Rosner S, Reuss JE, Zahurak M. Five-year clinical outcomes after neoadjuvant nivolumab in resectable non-small cell lung cancer. Clin Cancer Res.. 2023; 29:705-10. DOI | PubMed |
- Carbone D, Waqar S, Chaft J. 145MO Updated survival, efficacy and safety of adjuvant (adj) atezolizumab (atezo) after neoadjuvant (neoadj) atezo in the phase II LCMC3 study. J Thorac Oncol.. 2023; 18:S90-1. DOI
- Wislez M, Mazieres J, Lavole A. Neoadjuvant durvalumab for resectable non-small-cell lung cancer (NSCLC): results from a multicenter study (IFCT-1601 IONESCO). J Immunother Cancer.. 2022; 10:e005636. DOI | PubMed |
- Chaft JE, Oezkan F, Kris MG. ; LCMC study investigators. Neoadjuvant atezolizumab for resectable non-small cell lung cancer: an open-label, single-arm phase II trial. Nat Med.. 2022; 28:2155-61. DOI | PubMed |
- Gao S, Li N, Gao S. Neoadjuvant PD-1 inhibitor (Sintilimab) in NSCLC. J Thorac Oncol.. 2020; 15:816-26. DOI
- Cascone T, William WN, Weissferdt A. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: the phase 2 randomized NEOSTAR trial. Nat Med.. 2021; 27:504-14. DOI
- Cascone T, García-campelo R, Spicer J. Abstract CT011: NeoCOAST: open-label, randomized, phase 2, multidrug platform study of neoadjuvant durvalumab alone or combined with novel agents in patients (pts) with resectable, early-stage non-small-cell lung cancer (NSCLC). Cancer Res.. 2022; 82 Suppl:CT011. DOI
- Schuler M, Cuppens K, Plönes T. Neoadjuvant nivolumab with or without relatlimab in resectable non-small-cell lung cancer: a randomized phase 2 trial. Nat Med.. 2024; 30:1602-11. DOI | PubMed |
- Forde PM, Spicer J, Lu S. Neoadjuvant nivolumab plus chemotherapy in resectable lung cancer. N Engl J Med.. 2022; 386:1973-85. DOI | PubMed |
- Lei J, Zhao J, Gong L. Neoadjuvant camrelizumab plus platinum-based chemotherapy vs chemotherapy alone for Chinese patients with resectable stage IIIA or IIIB (T3N2) non-small cell lung cancer: the TD-FOREKNOW randomized clinical trial. JAMA Oncol.. 2023; 9:1348. DOI
- Aokage K, Shimada Y, Yoh K. Pembrolizumab and ramucirumab neoadjuvant therapy for PD-L1-positive stage IB-IIIA lung cancer (EAST ENERGY). J Clin Oncol.. 2023; 41:8509. DOI
- Zhao J, Zhao L, Guo W. Efficacy, Safety, and biomarker analysis of neoadjuvant camrelizumab and Apatinib in patients with resectable NSCLC: a phase 2 clinical trial. J Thorac Oncol.. 2023; 18:780-91. DOI
- Schvartsman G, Rezende ACPD, Gomes DBD. Stereotactic ablative radiotherapy with nivolumab for early-stage operable non-small cell lung cancer: a phase 2 study. J Clin Oncol.. 2023; 41:8554. DOI
- Altorki NK, Mcgraw TE, Borczuk AC. Neoadjuvant durvalumab with or without stereotactic body radiotherapy in patients with early-stage non-small-cell lung cancer: a single-centre, randomised phase 2 trial. Lancet Oncol.. 2021; 22:824-35. DOI
- Altorki NK, Walsh ZH, Melms JC. Neoadjuvant durvalumab plus radiation vs. durvalumab alone in stages I-III non-small cell lung cancer: survival outcomes and molecular correlates of a randomized phase II trial. Nat Commun.. 2023; 14:8435. DOI
- Zhao Z, Liu S, Zhou T. Stereotactic body radiation therapy with sequential immunochemotherapy as neoadjuvant therapy in resectable non-small cell lung cancer (SACTION-01 study). J Clin Oncol.. 2023; 41:8540. DOI
- Wakelee HA, Altorki NK, Zhou C. IMpower010: Primary results of a phase III global study of atezolizumab vs. best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). J Clin Oncol.. 2021; 39:8500. DOI
- Felip E, Altorki N, Zhou C. Overall survival with adjuvant atezolizumab after chemotherapy in resected stage II-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase III trial. Ann Oncol.. 2023; 34:907-19. DOI
- O’Brien M, Paz-Ares L, Marreaud S. Pembrolizumab vs. placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol.. 2022; 23:1274-86. DOI | PubMed
- Wakelee H, Liberman M, Kato T. Perioperative pembrolizumab for early-stage non-small-cell lung cancer. N Engl J Med.. 2023; 389:491-503. DOI | PubMed |
- Lu S, Zhang W, Wu L. ; Neotorch Investigators. Perioperative toripalimab plus chemotherapy for patients with resectable non-small cell lung cancer: the neotorch randomized clinical trial. JAMA.. 2024; 331:201. DOI
- Yue D, Wang W, Liu H. LBA58 Pathological response to neoadjuvant tislelizumab (TIS) plus platinum-doublet (PtDb) chemotherapy (CT) in resectable stage II-IIIA NSCLC patients (pts) in the phase III (Ph3) RATIONALE-315 trial. Ann Oncol.. 2023; 34:S1299. DOI
- Yue D, Wang W, Liu H. VP1-2024: RATIONALE-315: Event-free survival (EFS) and overall survival (OS) of neoadjuvant tislelizumab (TIS) plus chemotherapy (CT) with adjuvant TIS in resectable non-small cell lung cancer (NSCLC). Ann Oncol.. 2024; 35:332-3. DOI
- Yue D, Tan L, Xu S. 108O Surgical outcomes from RATIONALE-315: Randomized, double-blind, phase III study of perioperative tislelizumab with neoadjuvant chemotherapy in resectable NSCLC. ESMO Open.. 2024; 9:102687. DOI
- Cascone T, Provencio M, Sepesi B. Checkmate 77T: A phase III trial of neoadjuvant nivolumab (NIVO) plus chemotherapy (chemo) followed by adjuvant nivo in resectable early-stage NSCLC. J Clin Oncol.. 2020; 38:TPS9076. DOI
- Heymach JV, Harpole D, Mitsudomi T. Abstract CT005: AEGEAN: a phase 3 trial of neoadjuvant durvalumab + chemotherapy followed by adjuvant durvalumab in patients with resectable NSCLC. Cancer Res.. 2023; 83 Suppl:CT005. DOI
- Wang C, Wang M, Long H. 492P Penpulimab-based combination neoadjuvant/adjuvant therapy for patients with resectable locally advanced non-small cell lung cancer: preliminary results from a phase II study (ALTER-L043). Ann Oncol.. 2023; 34:S1655. DOI
- Li J, Li Q, Lu S, Jiang L, Li L, Xie S. MA16.05 Phase Ib trial of neoadjuvant low dose radiotherapy, chemotherapy, and durvalumab for potentially resectable stage III NSCLC. J Thorac Oncol.. 2023; 18:S158-9. DOI
- Mauti LA, Finazzi T, Holer L. SAKK 16/18: immune-modulatory radiotherapy to enhance the effects of neoadjuvant PD-L1 blockade after neoadjuvant chemotherapy in patients with resectable stage III (N2) non-small cell lung cancer (NSCLC) - a multicenter phase II trial. J Clin Oncol.. 2023; 41:8547. DOI
- Peters S, Kim A, Solomon B. IMpower030: Phase III study evaluating neoadjuvant treatment of resectable stage II-IIIB non-small cell lung cancer (NSCLC) with atezolizumab (atezo) + chemotherapy. Ann Oncol.. 2019; 30:ii30. DOI
- Lee J, Cho J, Lee C. Phase Ib study of neoadjuvant concurrent chemoradiation plus durvalumab followed by surgery and adjuvant durvalumab for resectable stage III NSCLC. J Clin Oncol.. 2023; 41:8556. DOI
- Antonia SJ, Villegas A, Daniel D. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med.. 2017; 377:1919-29. DOI
- Zhou Q, Chen M, Jiang O. Sugemalimab vs. placebo after concurrent or sequential chemoradiotherapy in patients with locally advanced, unresectable, stage III non-small-cell lung cancer in China (GEMSTONE-301): interim results of a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol.. 2022; 23:209-19. DOI
- Girard N, Bar J, Garrido P. Treatment characteristics and real-world progression-free survival in patients with unresectable stage III NSCLC who received durvalumab after chemoradiotherapy: findings from the PACIFIC-R study. J Thorac Oncol.. 2023; 18:181-93. DOI
- Garassino MC, Mazieres J, Reck M. Durvalumab after sequential chemoradiotherapy in stage III, unresectable NSCLC: the phase 2 PACIFIC-6 trial. J Thorac Oncol.. 2022; 17:1415-27. DOI
- Filippi AR, Dziadziuszko R, García Campelo MR, Paoli J, Sawyer W, Díaz Pérez IE. DUART: durvalumab after radiotherapy in patients with unresectable, stage III NSCLC who are ineligible for chemotherapy. Future Oncol.. 2021; 17:4657-63. DOI
- Bozorgmehr F, Buchmeier E, Hammer-hellmig M. 1293MO safety and efficacy of hypo- and conventionally fractionated thoracic radiotherapy plus durvalumab in elderly or frail NSCLC stage III patients unfit for chemotherapy: interim results from the TRADE-hypo trial. Ann Oncol.. 2023; 34:S746. DOI
- Herbst RS, Majem M, Barlesi F. COAST: an open-label, Phase II, multidrug platform study of durvalumab alone or in combination with oleclumab or monalizumab in patients with unresectable, stage III non-small-cell lung cancer. J Clin Oncol.. 2022; 40:3383-93. DOI
- Ross HJ, Kozono DE, Urbanic JJ. AFT-16: Phase II trial of neoadjuvant and adjuvant atezolizumab and chemoradiation (CRT) for stage III non-small cell lung cancer (NSCLC). J Clin Oncol.. 2021; 39:8513. DOI
- Wang Y, Zhang T, Wang J, Bi N. EP05.01-004 induction chemoimmunotherapy before definitive chemoradiotherapy for large-volume unresectable locally advanced NSCLC. J Thorac Oncol.. 2022; 17:S266-7. DOI
- Peters S, Felip E, Dafni U. Progression-free and overall survival for concurrent nivolumab with standard concurrent chemoradiotherapy in locally advanced stage IIIA-B NSCLC: results from the european thoracic oncology platform NICOLAS phase II trial (European Thoracic Oncology Platform 6-14). J Thorac Oncol.. 2021; 16:278-88. DOI
- Jabbour SK, Lee KH, Frost N. Pembrolizumab plus concurrent chemoradiation therapy in patients with unresectable, locally advanced, stage III non-small cell lung cancer: the phase 2 KEYNOTE-799 nonrandomized trial. JAMA Oncol.. 2021; 7:1351. DOI
- Chang JY, Lin SH, Dong W. Stereotactic ablative radiotherapy with or without immunotherapy for early-stage or isolated lung parenchymal recurrent node-negative non-small-cell lung cancer: an open-label, randomised, phase 2 trial. Lancet.. 2023; 402:871-81. DOI
- Lin SH, Lin Y, Yao L. Phase II trial of concurrent atezolizumab with chemoradiation for unresectable NSCLC. J Thorac Oncol.. 2020; 15:248-57. DOI
- Jabbour SK, Cho BC, Bria E. Rationale and design of the phase III KEYLYNK-012 study of pembrolizumab and concurrent chemoradiotherapy followed by pembrolizumab with or without Olaparib for stage III non-small-cell lung cancer. Clin Lung Cancer.. 2022; 23:e342-6. DOI | PubMed |
- Xing L, Yu J, Peters S. 167TiP AdvanTIG-301: Anti-TIGIT monoclonal antibody (mAb) ociperlimab (OCI) + tislelizumab (TIS) + concurrent chemoradiotherapy (cCRT) followed by OCI + TIS or TIS + cCRT followed by TIS vs cCRT followed by durvalumab (DUR) in previously untreated, locally advanced, unresectable NSCLC. Ann Oncol.. 2021; 32:S1455. DOI
- De Ruysscher D, Ramalingam S, Urbanic J. CheckMate 73L: A phase 3 study comparing nivolumab plus concurrent chemoradiotherapy followed by nivolumab with or without ipilimumab vs. concurrent chemoradiotherapy followed by durvalumab for previously untreated, locally advanced stage III non-small-cell lung cancer. Clin Lung Cancer.. 2022; 23:e264-8. DOI
- Socinski MA, Nishio M, Jotte RM. IMpower150 final overall survival analyses for atezolizumab plus bevacizumab and chemotherapy in first-line metastatic nonsquamous NSCLC. J Thorac Oncol.. 2021; 16:1909-24. DOI
- Herbst RS, Giaccone G, De Marinis F. Atezolizumab for first-line treatment of PD-L1–selected patients with NSCLC. N Engl J Med.. 2020; 383:1328-39. DOI
- Pacheco JM, Gao D, Camidge DR. Extended follow-up on KEYNOTE-024 suggests significant survival benefit for pembrolizumab in patients with PD-L1 ≥ 50%, but unanswered questions remain. Ann. Transl. Med.. 2019; 7 Suppl:S127. DOI | PubMed |
- Reck M, Rodríguez-Abreu D, Robinson AG. Updated analysis of KEYNOTE-024: pembrolizumab vs. platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol.. 2019; 37:537-46. DOI
- Mok TSK, Wu Y, Kudaba I. Pembrolizumab vs. chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet.. 2019; 393:1819-30. DOI
- Özgüroğlu M, Kilickap S, Sezer A. First-line cemiplimab monotherapy and continued cemiplimab beyond progression plus chemotherapy for advanced non-small-cell lung cancer with PD-L1 50% or more (EMPOWER-Lung 1): 35-month follow-up from a mutlicentre, open-label, randomised, phase 3 trial. Lancet Oncol.. 2023; 24:989-1001. DOI
- Paz-ares L, Luft A, Vicente D. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med.. 2018; 379:2040-51. DOI
- Novello S, Kowalski D, Luft A. 974MO 5-year update from KEYNOTE-407: pembrolizumab plus chemotherapy in squamous non-small cell lung cancer (NSCLC). Ann Oncol.. 2022; 33:S993-4. DOI
- Wang J, Lu S, Yu X. Tislelizumab plus chemotherapy vs chemotherapy alone as first-line treatment for advanced squamous non-small-cell lung cancer: a phase 3 randomized clinical trial. JAMA Oncol.. 2021; 7:709. DOI
- Ren S, Chen J, Xu X. Camrelizumab plus carboplatin and paclitaxel as first-line treatment for advanced squamous NSCLC (CameL-Sq): a phase 3 trial. J Thorac Oncol.. 2022; 17:544-57. DOI
- Zhou C, Cheng Y, Chen J. 3MO First-line camrelizumab plus carboplatin and paclitaxel for advanced squamous non-small cell lung cancer: updated overall survival results from the phase III CameL-sq trial. Ann Oncol.. 2022; 33:S28. DOI
- Zhou C, Ren S, Chen J. 62P First-line (1L) camrelizumab plus chemotherapy (chemo) for advanced squamous non-small cell lung cancer (sqNSCLC): 4-yr update from the phase III CameL-sq trial. ESMO Open.. 2024; 9:102641. DOI
- Zhou C, Wang Z, Sun M. Interim survival analysis of the randomized phase III GEMSTONE-302 trial: sugemalimab or placebo plus chemotherapy as first-line treatment for metastatic NSCLC. Nat Cancer.. 2023; 4:860-71. DOI | PubMed
- Zhong H, Sun S, Chen J. First-line penpulimab combined with paclitaxel and carboplatin for metastatic squamous non-small-cell lung cancer in China (AK105-302): a multicentre, randomised, double-blind, placebo-controlled phase 3 clinical trial. Lancet Resp Med.. 2024; 12:355-65. DOI
- Zhou C, Wu L, Fan Y. Sintilimab plus platinum and gemcitabine as first-line treatment for advanced or metastatic squamous NSCLC: results from a randomized, double-blind, phase 3 trial (ORIENT-12). J Thorac Oncol.. 2021; 16:1501-11. DOI
- Zhou C, Hu Y, Arkania E. A global phase 3 study of serplulimab plus chemotherapy as first-line treatment for advanced squamous non-small-cell lung cancer (ASTRUM-004). Cancer Cell.. 2024; 42:198-208.e3. DOI
- Makharadze T, Gogishvili M, Melkadze T. 50 Cemiplimab plus chemotherapy vs. chemotherapy alone in non-small cell lung cancer: longer follow-up results from the phase III EMPOWER-Lung 3 trial. J Thorac Oncol.. 2023; 18:S38-9. DOI
- Gogishvili M, Melkadze T, Makharadze T. Cemiplimab plus chemotherapy vs. chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial. Nat Med.. 2022; 28:2374-80. DOI | PubMed |
- Kilickap S, Sezer A, Özgüroğlu M. OA11.06 cemiplimab monotherapy for first line advanced NSCLC patients with PD-L1 expression ≥ 50%: 5-y outcomes of EMPOWER-Lung 1. J Thorac Oncol.. 2024; 19:S35. DOI | PubMed
- Paz-ares L, Ciuleanu T, Cobo M. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol.. 2021; 22:198-211. DOI
- Johnson ML, Cho BC, Luft A. ; for the POSEIDON investigators. Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: the phase III POSEIDON study. J Clin Oncol.. 2023; 41:1213-27. DOI
- Lee SM, Schulz C, Prabhash K. First-line atezolizumab monotherapy vs. single-agent chemotherapy in patients with non-small-cell lung cancer ineligible for treatment with a platinum-containing regimen (IPSOS): a phase 3, global, multicentre, open-label, randomised controlled study. Lancet.. 2023; 402:451-63. DOI
- Schoenfeld AJ, Rizvi HA, Memon D. Systemic and oligo-acquired resistance to PD-(L)1 blockade in lung cancer. Clin Cancer Res.. 2022; 28:3797-803. DOI
- Xuzhang W, Huang H, Yu Y, Shen L, Li Z, Lu S. Treatment strategies based on different oligoprogressive patterns after immunotherapy failure in metastatic NSCLC. Ther Adv Med Oncol.. 2023; 15:17588359231156387. DOI | PubMed |
- Xu Y, Li H, Fan Y. Progression patterns, treatment, and prognosis beyond resistance of responders to immunotherapy in advanced non-small cell lung cancer. Front. Oncol.. 2021; 11:642883. DOI | PubMed |
- Deng J, Yang M, Yang X, Chen Z, Xu C, Zhou Q. Patterns of failure and the subsequent treatment after progression on first-line immunotherapy monotherapy in advanced non-small cell lung cancer: a retrospective study. BMC Cancer.. 2024; 24:1190. DOI | PubMed |
- Grohé C, Wehler T, Dechow T. Nintedanib plus docetaxel after progression on first-line immunochemotherapy in patients with lung adenocarcinoma: cohort C of the non-interventional study, VARGADO. Transl Lung Cancer Res.. 2022; 11:2010-21. DOI | PubMed |
- Wu L, Fang Y, Pu X. Anlotinib plus docetaxel in advanced NSCLC progressing on immunotherapy: a pooled analysis of two randomized trials. J Clin Oncol.. 2024; 42:8062. DOI
- Katayama Y, Shimamoto T, Yamada T. Retrospective efficacy analysis of immune checkpoint inhibitor rechallenge in patients with non-small cell lung cancer. JCM.. 2019; 9:102. DOI | PubMed |
- Gobbini E, Toffart AC, Pérol M. Immune checkpoint inhibitors rechallenge efficacy in non-small-cell lung cancer patients. Clin Lung Cancer.. 2020; 21:e497-510. DOI | PubMed
- Giaj Levra M, Cotté F, Corre R. Immunotherapy rechallenge after nivolumab treatment in advanced non-small cell lung cancer in the real-world setting: a national data base analysis. Lung Cancer.. 2020; 140:99-106. DOI
- Herbst RS, Garon EB, Kim D. Long-term outcomes and retreatment among patients with previously treated, programmed death-ligand 1-positive, advanced non-small-cell lung cancer in the KEYNOTE-010 study. J Clin Oncol.. 2020; 38:1580-90. DOI | PubMed
- Sheth S, Gao C, Mueller N. Durvalumab activity in previously treated patients who stopped durvalumab without disease progression. J Immunother Cancer.. 2020; 8:e000650. DOI | PubMed |
- Aldea M, Andre F, Marabelle A, Dogan S, Barlesi F, Soria J. Overcoming resistance to tumor-targeted and immune-targeted therapies. Cancer Discov.. 2021; 11:874-99. DOI
- Kalbasi A, Ribas A. Tumour-intrinsic resistance to immune checkpoint blockade. Nat Rev Immunol.. 2019; 20:25-39. DOI | PubMed |
- Salous T, Shukla NA, Althouse SK. A phase 2 trial of chemotherapy plus pembrolizumab in patients with advanced non-small cell lung cancer previously treated with a PD‐1 or PD‐L1 inhibitor: big ten cancer research consortium BTCRC-LUN15-029. Cancer.. 2022; 129:264-71. DOI | PubMed
- Creelan B, Wang C, Teer J. Abstract CT056: Durable complete responses to adoptive cell transfer using tumor infiltrating lymphocytes (TIL) in non-small cell lung cancer (NSCLC): a phase I trial. Cancer Res.. 2020; 80 Suppl:CT056. DOI
- Kirkwood J, Zakharia Y, Davar D.DOI
- Reckamp KL, Redman MW, Dragnev KH. Overall survival from a phase II randomized study of ramucirumab plus pembrolizumab vs. standard of care for advanced non-small cell lung cancer previously treated with immunotherapy: lung-MAP nonmatched substudy S1800A. J Clin Oncol.. 2022; 40:9004. DOI | PubMed |
- Majem M, Forster M, Krebs M. 11MO Final data from a phase II study (TACTI-002) of eftilagimod alpha (soluble LAG-3) and pembrolizumab in 2nd-line metastatic NSCLC pts resistant to PD-1/PD-L1 inhibitors. J Thorac Oncol.. 2023; 18:S43-4. DOI
- Wu Y, Lu S, Cheng Y. Nivolumab vs. docetaxel in a predominantly Chinese patient population with previously treated advanced NSCLC: CheckMate 078 randomized phase III clinical trial. J Thorac Oncol.. 2019; 14:867-75. DOI
- Zhou C, Huang D, Fan Y. Tislelizumab vs. docetaxel in patients with previously treated advanced NSCLC (RATIONALE-303): a phase 3, open-label, randomized controlled trial. J Thorac Oncol.. 2023; 18:93-105. DOI | PubMed
- Herbst RS, Baas P, Kim D. Pembrolizumab vs. docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet.. 2016; 387:1540-50. DOI | PubMed
- Herbst RS, Garon EB, Kim D. Five year survival update from KEYNOTE-010: pembrolizumab vs. docetaxel for previously treated, programmed death-ligand 1-positive advanced NSCLC. J Thorac Oncol.. 2021; 16:1718-32. DOI | PubMed
- Rittmeyer A, Barlesi F, Waterkamp D. Atezolizumab vs. docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet.. 2017; 389:255-65. DOI
- Reck M, Rodríguez-Abreu D, Robinson AG. Five-year outcomes with pembrolizumab vs. chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50%. J Clin Oncol.. 2021; 39:2339-49. DOI
- Rodríguez-Abreu D, Powell S, Hochmair M. Pemetrexed plus platinum with or without pembrolizumab in patients with previously untreated metastatic nonsquamous NSCLC: protocol-specified final analysis from KEYNOTE-189. Ann Oncol.. 2021; 32:881-95. DOI
- Zhou C, Chen G, Huang Y. Camrelizumab plus carboplatin and pemetrexed as first-line treatment for advanced nonsquamous NSCLC: extended follow-up of CameL phase 3 Trial. J Thorac Oncol.. 2023; 18:628-39. DOI
- Yang Y, Wang Z, Fang J. Efficacy and safety of sintilimab plus pemetrexed and platinum as first-line treatment for locally advanced or metastatic nonsquamous NSCLC: a randomized, double-blind, phase 3 study (Oncology pRogram by InnovENT anti-PD-1-11). J Thorac Oncol.. 2020; 15:1636-46. DOI | PubMed
- Zhang L, Wang Z, Fang J. Final overall survival data of sintilimab plus pemetrexed and platinum as First-Line treatment for locally advanced or metastatic nonsquamous NSCLC in the Phase 3 ORIENT-11 study. Lung Cancer.. 2022; 171:56-60. DOI
- Lu S, Wang J, Yu Y. Tislelizumab plus chemotherapy as first-line treatment for locally advanced or metastatic nonsquamous NSCLC (RATIONALE 304): a randomized phase 3 trial. J Thorac Oncol.. 2021; 16:1512-22. DOI
- Zhou C, Wang Z, Sun Y. Sugemalimab vs. placebo, in combination with platinum-based chemotherapy, as first-line treatment of metastatic non-small-cell lung cancer (GEMSTONE-302): interim and final analyses of a double-blind, randomised, phase 3 clinical trial. Lancet Oncol. 2022;23:220-33.DOI
- Nishio M, Barlesi F, West H. Atezolizumab plus chemotherapy for first-line treatment of nonsquamous NSCLC: results from the randomized phase 3 IMpower132 trial. J Thorac Oncol.. 2021; 16:653-64. DOI
- Wang Z, Wu L, Li B. Toripalimab plus chemotherapy for patients with treatment-naive advanced non-small-cell lung cancer: a multicenter randomized phase III trial (CHOICE-01). J Clin Oncol.. 2023; 41:651-63. DOI | PubMed |
- West H, Mccleod M, Hussein M. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20:924-37.DOI
- Ramalingam S, Ciuleanu T, Bernabe Caro R. OA14.03 six-year survival and HRQoL outcomes with 1L nivolumab + ipilimumab in patients with metastatic NSCLC from CheckMate227. J Thorac Oncol.. 2023; 18:S76-7. DOI
- Cheng Y, Wu L, Fang Y. Abstract CT248: Trastuzumab deruxtecan (T-DXd) in Chinese patients (pts) with previously treated HER2 mutant non-small cell lung cancer (NSCLC): primary analysis from the Phase 2 DESTINY-Lung05 (DL-05) trial. Cancer Res.. 2024; 84 Suppl:CT248. DOI
- Felip E, Majem M, Doger B. A phase II study (TACTI-002) in first-line metastatic non-small cell lung carcinoma investigating eftilagimod alpha (soluble LAG-3 protein) and pembrolizumab: Updated results from a PD-L1 unselected population. J Clin Oncol.. 2022; 40:9003. DOI
- Forster M, Krebs M, Majem M. EP08.01-109 TACTI-002: A phase II study of Eftilagimod Alpha (Soluble LAG-3) & pembrolizumab in 2nd line PD-1/PD-L1 refractory metastatic NSCLC. J Thorac Oncol.. 2022; 17:S395. DOI
- Niu J, Maurice-Dror C, Lee D. First-in-human phase 1 study of the anti-TIGIT antibody vibostolimab as monotherapy or with pembrolizumab for advanced solid tumors, including non-small-cell lung cancer. Ann Oncol.. 2022; 33:169-80. DOI
- Cho BC, Abreu DR, Hussein M. Tiragolumab plus atezolizumab vs. placebo plus atezolizumab as a first-line treatment for PD-L1-selected non-small-cell lung cancer (CITYSCAPE): primary and follow-up analyses of a randomised, double-blind, phase 2 study. Lancet Oncol.2022;23:781-92.DOI
- Harding JJ, Moreno V, Bang Y. Blocking TIM-3 in treatment-refractory advanced solid tumors: a phase Ia/b study of LY3321367 with or without an anti-PD-L1 antibody. Clin Cancer Res.. 2021; 27:2168-78. DOI
- Zhao Y, Chen G, Chen J. AK112, a novel PD-1/VEGF bispecific antibody, in combination with chemotherapy in patients with advanced non-small cell lung cancer (NSCLC): an open-label, multicenter, phase II trial. eClinicalMedicine.. 2023; 62:102106. DOI | PubMed |
- Fang W, Zhao Y, Luo Y. ; HARMONi-A Study Investigators. Ivonescimab plus chemotherapy in non-small cell lung cancer With EGFR variant: a randomized clinical trial. JAMA.. 2024; 332:561. DOI | PubMed |
- Zhou C, Chen J, Wu L. PL02.04 Phase 3 study of Ivonescimab (AK112) vs. Pembrolizumab as first-line treatment for PD-L1-positive advanced NSCLC: primary analysis of HARMONi-2. J Thorac Oncol.. 2024; 19:S1. DOI
- Huang Y, Yang Y, Zhao Y. QL1706 (anti-PD-1 IgG4/CTLA-4 antibody) plus chemotherapy with or without bevacizumab in advanced non-small cell lung cancer: a multi-cohort, phase II study. Sig Transduct Target Ther.. 2024; 9:23. DOI | PubMed |
- Zhao Y, Chen G, Li X. KN046, a bispecific antibody against PD-L1 and CTLA-4, plus chemotherapy as first-line treatment for metastatic NSCLC: a multicenter phase 2 trial. Cell Reports Medicine.. 2024; 5:101470. DOI | PubMed |
- Feng J, Chen J, Li K. 1278P SHR-1701, a bifunctional fusion protein targeting PD-L1 and TGF-β, as first-line therapy for PD-L1+ advanced/metastatic NSCLC: Data from a clinical expansion cohort of a phase I study. Ann Oncol.. 2021; 32:S995. DOI
- Lu S, Wu L, Jian H. Sintilimab plus bevacizumab biosimilar IBI305 and chemotherapy for patients with EGFR-mutated non-squamous non-small-cell lung cancer who progressed on EGFR tyrosine-kinase inhibitor therapy (ORIENT-31): first interim results from a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol.. 2022; 23:1167-79. DOI
- Neal JW, Santoro A, Viteri S. Cabozantinib (C) plus atezolizumab (A) or C alone in patients (pts) with advanced non-small cell lung cancer (aNSCLC) previously treated with an immune checkpoint inhibitor (ICI): results from Cohorts 7 and 20 of the COSMIC-021 study. J Clin Oncol.. 2022; 40:9005. DOI
- Herbst RS, Arkenau H, Santana-davila R. Ramucirumab plus pembrolizumab in patients with previously treated advanced non-small-cell lung cancer, gastro-oesophageal cancer, or urothelial carcinomas (JVDF): a multicohort, non-randomised, open-label, phase 1a/b trial. Lancet Oncol.. 2019; 20:1109-23. DOI
- Gao G, Ni J, Wang Y. Efficacy and safety of camrelizumab plus apatinib in previously treated patients with advanced non-small cell lung cancer harboring EGFR or ALK genetic aberration. Transl Lung Cancer Res.. 2022; 11:964-74. DOI | PubMed |
- Chu T, Zhong R, Zhong H. Phase 1b study of sintilimab plus Anlotinib as first-line therapy in patients with advanced NSCLC. J Thorac Oncol.. 2021; 16:643-52. DOI
- Neal J, Pavlakis N, Kim S. CONTACT-01: a randomized phase III trial of atezolizumab + cabozantinib vs. docetaxel for metastatic non-small cell lung cancer after a checkpoint inhibitor and chemotherapy. J Clin Oncol.. 2024; 42:2393-403. DOI
- Herbst R, Cho B, Zhou C. 64O Lenvatinib plus pembrolizumab, pemetrexed, and a platinum (len + pembro + chemo) as first-line therapy for metastatic non squamous non-small cell lung cancer (NSCLC): Phase III LEAP-006 study. Immunooncol. Technol.. 2023; 20:100536. DOI
- Leighl N, Paz-Ares L, Abreu DR. 65O Phase III LEAP-008 study of lenvatinib plus pembrolizumab vs. docetaxel for metastatic non-small cell lung cancer (NSCLC) that progressed on a PD-(L)1 inhibitor and platinum-containing chemotherapy. Immunooncol. Technol.. 2023; 20:100537. DOI
- Borghaei H, Johnson M, Garon E. LBA63 SAPPHIRE: Phase III study of sitravatinib plus nivolumab vs. docetaxel in patients with previously treated advanced non-squamous non-small cell lung cancer (NSCLC). Ann Oncol.. 2023; 34:S1308. DOI
- Liu X, Deng J, Yuan Y. Advances in Trop2-targeted therapy: novel agents and opportunities beyond breast cancer. Pharmacol Ther.. 2022; 239:108296. DOI
- Inamura K, Yokouchi Y, Kobayashi M. Association of tumor TROP2 expression with prognosis varies among lung cancer subtypes. Oncotarget.. 2017; 8:28725-35. DOI | PubMed |
- Bessede A, Peyraud F, Besse B. TROP2 is associated with primary resistance to immune checkpoint inhibition in patients with advanced non-small cell lung cancer. Clin Cancer Res.. 2024; 30:779-85. DOI
- Cho B, Dols M, Reyes Cabanillas R. OA05.04 Sacituzumab Govitecan + Pembrolizumab in 1L metastatic non-small cell lung cancer: preliminary results of the EVOKE-02 study. J Thorac Oncol.. 2023; 18:S54. DOI
- Goto Y, Su W, Levy BP. TROPION-Lung02: Datopotamab deruxtecan (Dato-DXd) plus pembrolizumab (pembro) with or without platinum chemotherapy (Pt-CT) in advanced non-small cell lung cancer (aNSCLC). J Clin Oncol.. 2023; 41:9004. DOI
- Okamoto I, Kuyama S, Girard N. 1505TiP TROPION-Lung07: A phase III trial of datopotamab deruxtecan (Dato-DXd) plus pembrolizumab (pembro) with or without platinum chemotherapy (Pt-CT) as first-line (1L) therapy in advanced/metastatic (adv/met) non-small cell lung cancer (NSCLC) with PD-L1 expression. Ann Oncol.. 2023; 34:S847-8. DOI
- Levy BP, Felip E, Reck M. TROPION-Lung08: phase III study of datopotamab deruxtecan plus pembrolizumab as first-line therapy for advanced NSCLC. Future Oncol.. 2023; 19:1461-72. DOI
- Papadopoulos K, Bruno D, Kitazono S. OA05.06 Datopotamab deruxtecan (Dato-DXd) + durvalumab ± carboplatin in advanced/mNSCLC: initial results from phase 1b TROPION-Lung04. J Thorac Oncol.. 2023; 18:S55. DOI
- Fang W, Wang Q, Cheng Y. Sacituzumab tirumotecan (SKB264/MK-2870) in combination with KL-A167 (anti-PD-L1) as first-line treatment for patients with advanced NSCLC from the phase II OptiTROP-Lung01 study. J Clin Oncol.. 2024; 42:8502. DOI
- Smit EF, Felip E, Uprety D. Trastuzumab deruxtecan in patients with metastatic non-small-cell lung cancer (DESTINY-Lung01): primary results of the HER2-overexpressing cohorts from a single-arm, phase 2 trial. Lancet Oncol.. 2024; 25:439-54. DOI
- Goto K, Goto Y, Kubo T. Trastuzumab deruxtecan in patients with HER2-mutant metastatic non-small-cell lung cancer: primary results from the randomized, phase II DESTINY-Lung02 trial. J Clin Oncol.. 2024; 42:4852-63. DOI | PubMed |
- Society of Cancer Precision Medicine of Chinese Anti-Cancer Association; Lung Cancer Expert Group of Chinese Medical Journal. [Chinese expert consensus on immunotherapy for advanced non-small lung cancer with oncogenic driver mutations (2023 edition)]. Zhonghua Zhong Liu Za Zhi.. 2023; 45:717-40. DOI | PubMed
- Gettinger S, Hellmann MD, Chow LQ. Nivolumab plus erlotinib in patients with EGFR-mutant advanced NSCLC. J Thorac Oncol.. 2018; 13:1363-72. DOI
- Oxnard G, Yang J, Yu H. TATTON: a multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann Oncol.. 2020; 31:507-16. DOI
- Nogami N, Barlesi F, Socinski MA. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J Thorac Oncol.. 2022; 17:309-23. DOI
- Zhao Y, He Y, Wang W. Efficacy and safety of immune checkpoint inhibitors for individuals with advanced EGFR-mutated non-small-cell lung cancer who progressed on EGFR tyrosine-kinase inhibitors: a systematic review, meta-analysis, and network meta-analysis. Lancet Oncol.. 2024; 25:1347-56. DOI | PubMed
- Cho BC, Lu S, Felip E. Amivantamab plus lazertinib in previously untreated EGFR-mutated advanced NSCLC. N Engl J Med.. 2024; 391:1486-98. DOI | PubMed
- Passaro A, Wang J, Wang Y. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase III MARIPOSA-2 study. Ann Oncol.. 2024; 35:77-90. DOI | PubMed
- Russo A, Franchina T, Ricciardi G, Battaglia A, Picciotto M, Adamo V. Heterogeneous responses to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) in patients with uncommon EGFR mutations: new insights and future perspectives in this complex clinical scenario. Int J Mol Sci.. 2019; 20:1431. DOI | PubMed |
- Chinese Society of Clinical Oncology (CSCO) Non-small Cell Lung Cancer Committee. [Chinese expert consensus on non-small cell lung cancer with EGFR exon 20 insertion mutations (2023 edition)]. Zhongguo Fei Ai Za Zhi.. 2023; 26:325-37. DOI | PubMed |
- Kirchner M, Kluck K, Brandt R. The immune microenvironment in EGFR- and ERBB2-mutated lung adenocarcinoma. ESMO Open.. 2021; 6:100253. PubMed |
- Liu K, Li H, Tan Q. Tumor immune microenvironment of NSCLC with EGFR exon 20 insertions may predict efficacy of first-line ICI-combined regimen. Lung Cancer.. 2024; 195:107933. DOI
- Leal JL, Alexander M, Itchins M. EGFR exon 20 insertion mutations: clinicopathological characteristics and treatment outcomes in advanced non-small cell lung cancer. Clin Lung Cancer.. 2021; 22:e859-69. DOI | PubMed
- Li J, Xie M, Zhao R. Anti-angiogenic therapy or immunotherapy? A real-world study of patients with advanced non-small cell lung cancer with EGFR/HER2 exon 20 insertion mutations. Front. Oncol.. 2024; 14:1357231. DOI | PubMed |
- Choudhury NJ, Schoenfeld AJ, Flynn J. Response to standard therapies and comprehensive genomic analysis for patients with lung adenocarcinoma with EGFR exon 20 insertions. Clin Cancer Res.. 2021; 27:2920-7. DOI | PubMed |
- Zhou C, Tang K, Liu B. 513MO Amivantamab plus chemotherapy vs chemotherapy as a first-line treatment among Asian patients with EGFR exon 20 insertion-mutated advanced non-small cell lung cancer (NSCLC): PAPILLON subgroup analysis. Ann Oncol.. 2023; 34:S1668-9. DOI
- Xu Y, Yang JC, Chiu C. Efficacy and safety of sunvozertinib in treatment naïve NSCLC patients with EGFR exon20 insertion mutations. J Clin Oncol.. 2023; 41:9073. DOI
- Wang M, Fan Y, Sun M. Sunvozertinib for patients in China with platinum-pretreated locally advanced or metastatic non-small-cell lung cancer and EGFR exon 20 insertion mutation (WU-KONG6): single-arm, open-label, multicentre, phase 2 trial. Lancet Resp Med.. 2024; 12:217-24. DOI
- Park K, Haura EB, Leighl NB. Amivantamab in EGFR exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: initial results from the CHRYSALIS phase I study. J Clin Oncol.. 2021; 39:3391-402. DOI | PubMed |
- Riely GJ, Wood DE, Ettinger DS. Non-Small Cell Lung Cancer, Version 4.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw.. 2024; 22:249-74. DOI | PubMed
- Mazieres J, Drilon A, Lusque A. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol.. 2019; 30:1321-8. DOI | PubMed |
- Chinese expert consensus on immunotherapy for advanced non-small cell lung cancer with oncogenic driver mutations (2023 edition). Chin. Med. J.. 2024; 137:1016-8. DOI
- Jahanzeb M, Lin HM, Pan X, Yin Y, Baumann P, Langer CJ. Immunotherapy treatment patterns and outcomes among ALK-positive patients with non-small-cell lung cancer. Clin Lung Cancer.. 2021; 22:49-57. DOI | PubMed
- Gainor JF, Shaw AT, Sequist LV. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res.. 2016; 22:4585-93. DOI | PubMed |
- Gadgeel S, Dziubek K, Nagasaka M. OA09.03 pembrolizumab in combination with platinum-based chemotherapy in recurrent EGFR/ALK-positive non-small cell lung cancer (NSCLC). J Thorac Oncol.. 2021; 16:S863. DOI
- Lee GD, Lee SE, Oh D. MET exon 14 skipping mutations in lung adenocarcinoma: clinicopathologic implications and prognostic values. J Thorac Oncol.. 2017; 12:1233-46. DOI
- Chinese Society of Pathology; Pathology Quality Control Center; Lung Cancer Group of Chinese Medical Association Chinese Society of Oncology; China Anti-cancer Association Chinese Society of Lung Cancer; Chinese Thoracic Oncology Group. [Chinese expert consensus on clinical practice of MET detection in non-small cell lung cancer]. Zhonghua Bing Li Xue Za Zhi.. 2022; 51:1094-103. DOI | PubMed
- Lu S, Fang J, Li X. Once-daily savolitinib in Chinese patients with pulmonary sarcomatoid carcinomas and other non-small-cell lung cancers harbouring MET exon 14 skipping alterations: a multicentre, single-arm, open-label, phase 2 study. Lancet Respir Med.. 2021; 9:1154-64. DOI
- Yang J, Zhang Y, Wu L. 1379P Preliminary results of phase II KUNPENG study of vebreltinib in patients (Pts) with advanced NSCLC harboring c-MET alterations. Ann Oncol.. 2023; 34:S791. DOI
- Wolf J, Garon EB, Groen HJ. Capmatinib in MET exon 14-mutated, advanced NSCLC: Updated results from the GEOMETRY mono-1 study. J Clin Oncol.. 2021; 39:9020. DOI
- Sabari J, Leonardi G, Shu C. PD-L1 expression, tumor mutational burden, and response to immunotherapy in patients with MET exon 14 altered lung cancers. Ann Oncol.. 2018; 29:2085-91. DOI | PubMed |
- Han Y, Chen S, Xiang C. MA05.07 Intertumoral molecular heterogeneity of non-small cell lung cancer with MET exon 14 skipping. J Thorac Oncol.. 2022; 17:S60-1. DOI
- Kron A, Scheffler M, Heydt C. Genetic heterogeneity of MET-aberrant NSCLC and its impact on the outcome of immunotherapy. J Thorac Oncol.. 2021; 16:572-82. DOI
- Kohno T, Nakaoku T, Tsuta K. Beyond ALK-RET, ROS1 and other oncogene fusions in lung cancer. Transl Lung Cancer Res.. 2015; 4:156-64. DOI | PubMed |
- Lee J, Ku BM, Shim JH. Characteristics and outcomes of RET-rearranged Korean non-small cell lung cancer patients in real-world practice. Jpn J Clin Oncol.. 2020; 50:594-601. DOI
- Zhou C, Solomon B, Loong HH. First-line selpercatinib or chemotherapy and pembrolizumab in RET fusion-positive NSCLC. N Engl J Med.. 2023; 389:1839-50. DOI | PubMed |
- Knetki-Wróblewska M, Wojas-Krawczyk K, Kowalski DM, Krzakowski M. Non-small-cell lung cancer patients with coexistence of high PD-L1 expression and RET fusion - which path should we follow? case reports and literature review. JCM.. 2022; 11:1630. DOI | PubMed |
- Zhou C, Li C, Luo L. Anti-tumor efficacy of HRS-4642 and its potential combination with proteasome inhibition in KRAS G12D-mutant cancer. Cancer Cell.. 2024; 42:1286-1300.e8. DOI
- Wang X, Allen S, Blake JF. Identification of MRTX1133, a noncovalent, potent, and selective KRASG12D inhibitor. J Med Chem.. 2021; 65:3123-33. DOI | PubMed
- Borghaei H, Gettinger S, Vokes EE. Five-year outcomes from the randomized, phase III trials CheckMate 017 and 057: nivolumab vs. docetaxel in previously treated non-small-cell lung cancer. J Clin Oncol.. 2021; 39:723-33. DOI | PubMed |
- West HJ, Mccleland M, Cappuzzo F. Clinical efficacy of atezolizumab plus bevacizumab and chemotherapy in KRAS-mutated non-small cell lung cancer with STK11, KEAP1, or TP53 comutations: subgroup results from the phase III IMpower150 trial. J Immunother Cancer.. 2022; 10:e003027. DOI | PubMed |
- Gadgeel S, Rodriguez-Abreu D, Felip E. KRAS mutational status and efficacy in KEYNOTE-189: Pembrolizumab (pembro) plus chemotherapy (chemo) vs placebo plus chemo as first-line therapy for metastatic non-squamous NSCLC. Ann Oncol.. 2019; 30:xi64-5. DOI
- Herbst R, Lopes G, Kowalski D. LBA4 Association of KRAS mutational status with response to pembrolizumab monotherapy given as first-line therapy for PD-L1-positive advanced non-squamous NSCLC in Keynote-042. Ann Oncol.. 2019; 30:xi63-4. DOI
- Society of Cancer Precision Medicine of Chinese Anti-Cancer Association; Lung Cancer Expert Group of Chinese Medical Journal. [Chinese expert consensus on immunotherapy for advanced non-small lung cancer with oncogenic driver mutations (2022 edition)]. Zhonghua Zhong Liu Za Zhi.. 2022; 44:1047-65. DOI | PubMed
- Amanam I, Mambetsariev I, Gupta R. Role of immunotherapy and co-mutations on KRAS-mutant non- small cell lung cancer survival. J Thorac Dis.. 2020; 12:5086-95. DOI | PubMed |
- Dong Z, Zhong W, Zhang X. Potential predictive value of TP53 and KRAS mutation status for response to PD-1 blockade immunotherapy in lung adenocarcinoma. Clin Cancer Res.. 2017; 23:3012-24. DOI | PubMed
- Skoulidis F, Goldberg ME, Greenawalt DM. STK11/LKB1 mutations and PD-1 inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discov.. 2018; 8:822-35. DOI
- Adderley H, Blackhall FH, Lindsay CR. KRAS-mutant non-small cell lung cancer: converging small molecules and immune checkpoint inhibition. EBioMedicine.. 2019; 41:711-6. DOI | PubMed |
- Papillon-Cavanagh S, Doshi P, Dobrin R, Szustakowski J, Walsh AM. STK11 and KEAP1 mutations as prognostic biomarkers in an observational real-world lung adenocarcinoma cohort. ESMO Open.. 2020; 5:e000706. DOI | PubMed |
- Ricciuti B, Arbour KC, Lin JJ. Diminished efficacy of programmed death-(Ligand)1 inhibition in STK11- and KEAP1-mutant lung adenocarcinoma is affected by KRAS mutation status. J Thorac Oncol.. 2022; 17:399-410. DOI | PubMed |
- Jeong Y, Hoang NT, Lovejoy A. Role of KEAP1/NRF2 and TP53 mutations in lung squamous cell carcinoma development and radiation resistance. Cancer Discov.. 2017; 7:86-101. DOI | PubMed |
- Wiesweg M, Preuß C, Roeper J. BRAF mutations and BRAF mutation functional class have no negative impact on the clinical outcome of advanced NSCLC and associate with susceptibility to immunotherapy. Eur J Cancer.. 2021; 149:211-21. DOI
- Dudnik E, Peled N, Nechushtan H. BRAF mutant lung cancer: programmed death ligand 1 expression, tumor mutational burden, microsatellite instability status, and response to immune check-point inhibitors. J Thorac Oncol.. 2018; 13:1128-37. DOI
- Garcia-illescas D, Callejo A, Iranzo P. EP08.01-078 clinical outcomes in metastatic non-small cell lung cancer harboring BRAF mutations treated with immune checkpoint inhibitors. J Thorac Oncol.. 2022; 17:S378-9. DOI
- Planchard D, Besse B, Groen HJ. Phase 2 study of dabrafenib plus trametinib in patients with BRAF V600E-mutant metastatic NSCLC: updated 5-year survival rates and genomic analysis. J Thorac Oncol.. 2022; 17:103-15. DOI
- Riely GJ, Smit EF, Ahn M. Phase II, Open-label study of encorafenib plus binimetinib in patients with BRAFV600-mutant metastatic non-small-cell lung cancer. J Clin Oncol.. 2023; 41:3700-11. DOI | PubMed
- Makarem M, Ricciuti B, Alessi J. 2198P Clinicopathologic characteristics and outcomes to immune checkpoint inhibitor therapy in patients with HER2-altered metastatic non-small cell lung cancer. Ann Oncol.. 2023; 34:S1136. DOI
- Doebele RC, Drilon A, Paz-Ares L. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1-2 trials. Lancet Oncol.. 2020; 21:271-82. DOI | PubMed |
- Repetto M, Chiara Garassino M, Loong HH. NTRK gene fusion testing and management in lung cancer. Cancer Treat Rev.. 2024; 127:102733. DOI
- Zhao R, Yao F, Xiang C. Identification of NTRK gene fusions in lung adenocarcinomas in the Chinese population. J. Pathol.. 2021; 7:375-84. DOI | PubMed |
- Jonna S, Feldman RA, Swensen J. Detection of NRG1 gene fusions in solid tumors. Clin Cancer Res.. 2019; 25:4966-72. DOI
- Dudnik E, Bshara E, Grubstein A. Rare targetable drivers (RTDs) in non-small cell lung cancer (NSCLC): outcomes with immune check-point inhibitors (ICPi). Lung Cancer.. 2018; 124:117-24. DOI
- Zhang L, Liu H, Tian Y, Wang H, Yang X. A novel NCOR2-NTRK1 fusion detected in a patient of lung adenocarcinoma and response to larotrectinib: a case report. BMC Pulm Med.. 2021; 21:125. DOI | PubMed |
- Rosen EY, Goldman DA, Hechtman JF. TRK fusions are enriched in cancers with uncommon histologies and the absence of canonical driver mutations. Clin Cancer Res.. 2020; 26:1624-32. DOI
- Gatalica Z, Xiu J, Swensen J, Vranic S. Molecular characterization of cancers with NTRK gene fusions. Mod Pathol.. 2019; 32:147-53. DOI
- Suh K, Kang A, Ko G, Williamson T, Liao N, Sullivan SD. Projecting long-term clinical outcomes with larotrectinib compared with immune checkpoint inhibitors in metastatic nonsmall cell lung cancer and differentiated thyroid cancer. JMCP.. 2024; 30:581-7. DOI | PubMed |
- Xu C, Wang Q, Wang D. Expert consensus on the diagnosis and treatment of NRG1/2 gene fusion solid tumors. Glob. Med. Genet.. 2024; 11:86-99. DOI | PubMed |
- Schram A, Goto K, Kim D. 1315MO Durable efficacy of zenocutuzumab, a HER2 x HER3 bispecific antibody, in advanced NRG1 fusion-positive (NRG1+) non-small cell lung cancer (NSCLC). Ann Oncol.. 2023; 34:S756-7. DOI
- Drilon A, Duruisseaux M, Han J. Clinicopathologic Features and Response to Therapy of NRG1 fusion-driven lung cancers: the eNRGy1 global multicenter registry. J Clin Oncol.. 2021; 39:2791-802. DOI | PubMed |
- Krook MA, Reeser JW, Ernst G. Fibroblast growth factor receptors in cancer: genetic alterations, diagnostics, therapeutic targets and mechanisms of resistance. Br J Cancer.. 2020; 124:880-92. DOI | PubMed |
- Flockerzi FA, Roggia C, Langer F, Holleczek B, Bohle RM. FGFR1 gene amplification in squamous cell carcinomas of the lung: a potential favorable prognostic marker for women and for patients with advanced cancer. Virchows Arch.. 2017; 472:759-69. DOI
- Subbiah V, Iannotti N, Gutierrez M. FIGHT-101, a first-in-human study of potent and selective FGFR 1-3 inhibitor pemigatinib in pan-cancer patients with FGF/FGFR alterations and advanced malignancies. Ann Oncol.. 2022; 33:522-33. DOI | PubMed |
- Yang C, Song D, Zhao F. Comprehensive analysis of the prognostic value and immune infiltration of FGFR family members in gastric cancer. Front. Oncol.. 2022; 12:936952. DOI | PubMed |
- Zhang W, Xia H, Yang R. Fibroblast growth factor receptor family mutations as a predictive biomarker for immune checkpoint inhibitors and its correlation with tumor immune microenvironment in melanoma. Front. Immunol.. 2022; 13:1030969. DOI | PubMed |
- Wu Y, Yi Z, Li J. FGFR blockade boosts T cell infiltration into triple-negative breast cancer by regulating cancer-associated fibroblasts. Theranostics.. 2022; 12:4564-80. DOI | PubMed |
- Santiago-walker AE, Chen F, Loriot Y. Predictive value of fibroblast growth factor receptor (FGFR) mutations and gene fusions on anti-PD-(L)1 treatment outcomes in patients (pts) with advanced urothelial cancer (UC). J Clin Oncol.. 2019; 37:419. DOI
- Benjamin DJ, Mar N, Rezazadeh Kalebasty A. Immunotherapy with checkpoint inhibitors in FGFR-altered urothelial carcinoma. Clin Med Insights Oncol.. 2022; 16:11795549221126252. DOI | PubMed |
- Gao G, Cui L, Zhou F. Special issue “The advance of solid tumor research in China”: FGFR4 alterations predict efficacy of immune checkpoint inhibitors in nonsmall cell lung cancer. Int J Cancer.. 2022; 152:79-89. DOI | PubMed
- Yi C, Chen L, Lin Z. Lenvatinib targets FGF receptor 4 to enhance antitumor immune response of anti-programmed cell death‐1 in HCC. Hepatology.. 2021; 74:2544-60. DOI | PubMed
- Palakurthi S, Kuraguchi M, Zacharek SJ. The combined effect of FGFR inhibition and PD-1 blockade promotes tumor-intrinsic induction of antitumor immunity. Cancer Immunology Research.. 2019; 7:1457-71. DOI
- Atkins MB, Ascierto PA, Feltquate D. Society for Immunotherapy of Cancer (SITC) consensus definitions for resistance to combinations of immune checkpoint inhibitors with targeted therapies. J Immunother Cancer.. 2023; 11:e005923. DOI | PubMed |
- Committee of Non-Small Cell Lung Cancer of Chinese Society of Clinical Oncology. [Chinese expert consensus on evaluation and treatment of advanced non-small cell lung cancer with negative driver genes after first-line immunotherapy resistance (2024 edition)]. Zhonghua Yi Xue Za Zhi.. 2024; 104:411-26. DOI | PubMed
- Seymour L, Bogaerts J, Perrone A. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol.. 2017; 18:e143-52. DOI
- Guan Y, Feng D, Yin B, Li K, Wang J. Immune-related dissociated response as a specific atypical response pattern in solid tumors with immune checkpoint blockade. Ther Adv Med Oncol.. 2022; 14:17588359221096877. DOI | PubMed |
- Onesti CE, Frères P, Jerusalem G. Atypical patterns of response to immune checkpoint inhibitors: interpreting pseudoprogression and hyperprogression in decision making for patients’ treatment. J. Thorac. Dis.. 2019; 11:35-8. DOI | PubMed |
- Waxman ES, Lee Gerber D. Pseudoprogression and immunotherapy phenomena. J Adv Pract Oncol.. 2020; 11:723-31. DOI | PubMed |
- Wang Q, Gao J, Wu X. Pseudoprogression and hyperprogression after checkpoint blockade. Int Immunopharmacol.. 2018; 58:125-35. DOI
- Champiat S, Ferrara R, Massard C. Hyperprogressive disease: recognizing a novel pattern to improve patient management. Nat Rev Clin Oncol.. 2018; 15:748-62. DOI
- Borcoman E, Kanjanapan Y, Champiat S. Novel patterns of response under immunotherapy. Ann Oncol.. 2019; 30:385-96. DOI
- Champiat S, Dercle L, Ammari S. Hyperprogressive disease is a new pattern of progression in cancer patients treated by anti-PD-1/PD-L1. Clin Cancer Res.. 2017; 23:1920-8. DOI
- Kanjanapan Y, Day D, Wang L. Hyperprogressive disease in early‐phase immunotherapy trials: clinical predictors and association with immune‐related toxicities. Cancer.. 2019; 125:1341-9. DOI
- Ferrara R, Mezquita L, Texier M. Hyperprogressive disease in patients with advanced non-small cell lung cancer treated with PD-1/PD-L1 inhibitors or with single-agent chemotherapy. JAMA Oncol.. 2018; 4:1543. DOI | PubMed |
- Kato S, Goodman A, Walavalkar V, Barkauskas DA, Sharabi A, Kurzrock R. Hyperprogressors after immunotherapy: analysis of genomic alterations associated with accelerated growth rate. Clin Cancer Res.. 2017; 23:4242-50. DOI
- Eisenhauer E, Therasse P, Bogaerts J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer.. 2009; 45:228-47. DOI
- Marabelle A, Le DT, Ascierto PA. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer: results from the phase II KEYNOTE-158 study. J Clin Oncol.. 2020; 38:1-10. DOI | PubMed |
- Mok T, Lopes G, Cho B. Associations of tissue tumor mutational burden and mutational status with clinical outcomes in KEYNOTE-042: pembrolizumab vs. chemotherapy for advanced PD-L1-positive NSCLC. Ann Oncol.. 2023; 34:377-88. DOI
- Ricciuti B, Wang X, Alessi JV. Association of high tumor mutation burden in non-small cell lung cancers with increased immune infiltration and improved clinical outcomes of PD-L1 blockade across PD-L1 expression levels. JAMA Oncol.. 2022; 8:1160. DOI | PubMed |
- Sesma A, Pardo J, Cruellas M. From tumor mutational burden to blood T cell receptor: looking for the best predictive biomarker in lung cancer treated with immunotherapy. Cancers.. 2020; 12:2974. DOI | PubMed |
- Hause RJ, Pritchard CC, Shendure J, Salipante SJ. Erratum: Corrigendum: classification and characterization of microsatellite instability across 18 cancer types. Nat Med.. 2017; 23:1241. DOI | PubMed
- De Marchi P, Berardinelli GN, Cavagna R. EP1.04-11 frequency of microsatellite instability (MSI) in Brazilian TKI non-treatable non-small cell lung cancer (NSCLC) patients. J Thorac Oncol.. 2019; 14:S973. DOI
- Qin J, Shi D, Yin Y. The clinical and genomic characteristics of MSI-h/dMMR lung cancer. J Clin Oncol.. 2022; 40:e21142. DOI
- Olivares-hernández A, Del Barco Morillo E, Parra Pérez C. Influence of DNA mismatch repair (MMR) system in survival and response to immune checkpoint inhibitors (ICIs) in non-small cell lung cancer (NSCLC): retrospective analysis. Biomedicines.. 2022; 10:360. DOI | PubMed |
- Li N, Wan Z, Lu D, Chen R, Ye X. Long-term benefit of immunotherapy in a patient with squamous lung cancer exhibiting mismatch repair deficient/high microsatellite instability/high tumor mutational burden: a case report and literature review. Front. Immunol.. 2023; 13:1088683. DOI | PubMed |
- Le DT, Uram JN, Wang H. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med.. 2015; 372:2509-20. DOI
- Gataa I, Mezquita L, Rossoni C. Tumour-infiltrating lymphocyte density is associated with favourable outcome in patients with advanced non-small cell lung cancer treated with immunotherapy. Eur J Cancer.. 2021; 145:221-9. DOI | PubMed
- Ballot E, Ladoire S, Routy B, Truntzer C, Ghiringhelli F. Tumor infiltrating lymphocytes signature as a new pan-cancer predictive biomarker of anti PD-1/PD-L1 efficacy. Cancers.. 2020; 12:2418. DOI | PubMed |
- Sun D, Liu J, Zhou H. Classification of tumor immune microenvironment according to programmed death-ligand 1 expression and immune infiltration predicts response to immunotherapy plus chemotherapy in advanced patients with NSCLC. J Thorac Oncol.. 2023; 18:869-81. DOI
- Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov.. 2019; 18:197-218. DOI
- Cui S, Dong L, Qian J, Ye L, Jiang L. Classifying non-small cell lung cancer by status of programmed cell death ligand 1 and tumor-infiltrating lymphocytes on tumor cells. J. Cancer.. 2018; 9:129-34. DOI | PubMed |
- Teng MW, Ngiow SF, Ribas A, Smyth MJ. Classifying cancers based on T-cell infiltration and PD-L1. Cancer Res.. 2015; 75:2139-45. DOI
- Kim ES, Velcheti V, Mekhail T. Blood-based tumor mutational burden as a biomarker for atezolizumab in non-small cell lung cancer: the phase 2 B-F1RST trial. Nat Med.. 2022; 28:939-45. DOI | PubMed |
- Chalabi M, Cardona A, Nagarkar D. Efficacy of chemotherapy and atezolizumab in patients with non-small-cell lung cancer receiving antibiotics and proton pump inhibitors: pooled post hoc analyses of the OAK and POPLAR trials. Ann Oncol.. 2020; 31:525-31. DOI
- Routy B, Le Chatelier E, Derosa L. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science.. 2018; 359:91-7. DOI | PubMed
- Esfahani K, Elkrief A, Calabrese C. Moving towards personalized treatments of immune-related adverse events. Nat Rev Clin Oncol.. 2020; 17:504-15. DOI
- Suijkerbuijk KPM, Van Eijs MJM, Van Wijk F, Eggermont AMM. Clinical and translational attributes of immune-related adverse events. Nat Cancer.. 2024; 5:557-71. DOI
- Martins F, Sofiya L, Sykiotis GP. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nat Rev Clin Oncol.. 2019; 16:563-80. DOI
- Xu C, Chen Y, Du X. Comparative safety of immune checkpoint inhibitors in cancer: systematic review and network meta-analysis. BMJ.. 2018;k4226. DOI | PubMed |
- Eigentler TK, Hassel JC, Berking C. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat Rev.. 2016; 45:7-18. DOI
- Zhou X, Yao Z, Bai H. Treatment-related adverse events of PD-1 and PD-L1 inhibitor-based combination therapies in clinical trials: a systematic review and meta-analysis. Lancet Oncol.. 2021; 22:1265-74. DOI
- Wang Y, Zhou S, Yang F. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol.. 2019; 5:1008. DOI | PubMed |
- Lam T, Tsang K, Choi H. Combination atezolizumab, bevacizumab, pemetrexed and carboplatin for metastatic EGFR mutated NSCLC after TKI failure. Lung Cancer.. 2021; 159:18-26. DOI
- Mok T, Nakagawa K, Park K. Nivolumab plus chemotherapy in epidermal growth factor receptor-mutated metastatic non-small-cell lung cancer after disease progression on epidermal growth factor receptor tyrosine kinase inhibitors: final results of CheckMate 722. J Clin Oncol.. 2024; 42:1252-64. DOI | PubMed |
- Yang JC, Lee DH, Lee J. Pemetrexed and platinum with or without pembrolizumab for tyrosine kinase inhibitor (TKI)-resistant, EGFR-mutant, metastatic nonsquamous NSCLC: phase 3 KEYNOTE-789 study. J Clin Oncol.. 2023; 41:LBA9000. DOI
- Jiang T, Wang P, Zhang J. Toripalimab plus chemotherapy as second-line treatment in previously EGFR-TKI treated patients with EGFR-mutant-advanced NSCLC: a multicenter phase-II trial. Sig Transduct Target Ther.. 2021; 6:355. DOI | PubMed |
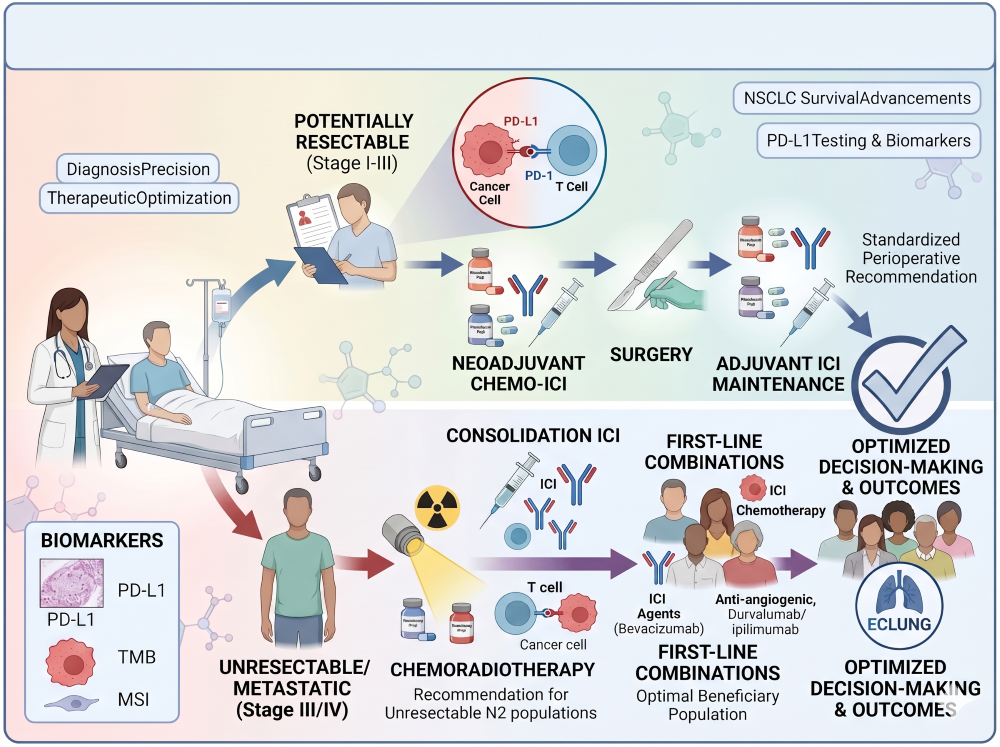
Additional Files
Published
Issue
Section
License
Copyright (c) 2026 Chunwei Xu, Danru Zheng, Qian Wang, Wenxian Wang, Dong Wang, Fangcen Lan, Jinpu Yu, Wenzhao Zhong, Zhijie Wang, Wenfeng Fang, Yongchang Zhang, Jingjing Liu, Shirong Zhang, Yu Zhang, Anwen Liu, Wen Liu, Ping Zhan, Hongbing Liu, Tangfeng Lv, Liyun Miao, Lingfeng Min, Gen Lin, Jingping Yuan, Zhansheng Jiang, Long Huang, Xingxiang Pu, Chuangzhou Rao, Dongqing Lv, Zongyang Yu, Xiaoyan Li, Chuanhao Tang, Chengzhi Zhou, Junping Zhang, Hui Guo, Qian Chu, Rui Meng, Jingxun Wu, Jin Zhou, Zhengfei Zhu, Xiaofeng Chen, Weiwei Pan, Xuewen Liu, Fei Pang, Kai Wang, Fan Wu, Bingwei Xu, Liping Wang, Youcai Zhu, Yanhong Shang, Jianfei Tu, Xinqing Lin, Jing Cai, Ling Xu, Jisheng Li, Xiaodong Jiao, Kainan Li, Huijing Feng, Lin Wang, Yingying Du, Yao Wang, Xuefei Shi, Xiaomin Niu, Dongmei Yuan, Yanwen Yao, Jianhui Huang, Yinbin Zhang, Pingli Sun, Hong Wang, Mingxiang Ye, Zhaofeng Wang, Yue Hao, Jin Kang, Jiatao Zhang, Chao Zhang, Wenbin Gao, Zhen Wang, Bin Wan, Donglai Lv, Shengjie Yang, Lin Shi, Yina Wang, Bihui Li, Zhang Zhang, Zhefeng Liu, Nong Yang, Lin Wu, Huijuan Wang, Xuelei Ma, Guansong Wang, Jiandong Wang, Meiyu Fang, Yong Fang, Yuan Li, Ke Wang, Yiping Zhang, Xixu Zhu, Yi Shen, Shenglin Ma, Yuanzhi Lu, Song Yong, Ziming Li, Zhengbo Song, Xiuyu Cai (Author)

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.